universitatea de medicina si farmacie “gr.t.popa” facultatea de … doctorat/rezumat... ·...
TRANSCRIPT
UNIVERSITATEA DE MEDICINA SI FARMACIE “GR.T.POPA”
FACULTATEA DE MEDICINĂ
Tratamentul Imunomodulator Actual al Sclerozei Multiple
Teza de Doctorat- Resumat
Conducator Stiintific Doctorand Prof. univ. Dr. Cristian Dinu Popescu Mitropoulou Efstathia
Iasi 2012
Table of contents
I. Introduction------------------------------------------1
II. Therapies applied on MS patients---------------5
III. Material and Method-----------------------------24
IV. Meeting our Variables by observing our
patients before the initiation of treatment----26
V. Immunomodulation- general review-----------35
VI. Avonex, Rebif, Betaseron and Copaxone
treated- groups of patients: Special
characteristics and metanalysis-----------------48
VII. References-------------------------------------------60
Resume
1
General Part Introduction
Multiple sclerosis is a chronic, inflammatory
demyelinating, neurodegenerative disease of the central nervous system, which affects 2.5 million people around the world. MS appears more frequently among young adults; it is uncommon before adolescence and also distinctly unusual after the age of 60. Multiple sclerosis occurs more frequently in women than men, with a female to male sex ratio calculated approximately 1.8:1, after 30 incidence-prevalence studies. This ratio is affected by the geographical distribution. According to Barlow, Kurtzke and colleagues, the disease is more common between the latitudes 30-35° northern and also 30-35° southern and its prevalence increases proportionally with the distance from equator in both hemispheres. Racial differences play also a significant role in the development of MS and may persist regardless the geography. Asians and Africans have a low prevalence rate, in contrary with Caucasians, especially those of the northern European descend.
There are some risk factors that trigger the appearance of the disease. For example, environmental factors like cold climate, humidity, hours of daily sunshine, amount of peat in soil, resistance to certain viruses, consumption of cow’s milk, other dietary factors
Resume
2
like meat consumption. Additionally, there is a risk in developing MS in families with one or more members affected. While in general population the prevalence of MS is about 0.1%, among the first degree relatives of MS patients this prevalence is 3-4% (25-50 times higher) (6). More precisely, 15% of MS patients have a relative who also suffers from the disease. The risk is increased in siblings (3%), slightly lower in parents and children (2%) and less than 2% for second and third degree relatives. Furthermore, genes seem to influence the severity of the disease or other types of the clinical phenotype. This observation, combined with pedigree data from families with more than one affected member and twins suggest that multiple unlinked genes predispose to the development of MS (polygenic inheritance). Each of these loci has a small contribution to the overall risk of developing the disease. The effect of these genes may be influenced by interactions with other genes and by the specific environmental exposures. Two genes, HLA-DRB1 and IL7R (CD127), have been unambiguously associated with disease susceptibility and/or protection following their identification as candidates by function. Almost 50% of patients carry the –DR2 gene and its corresponding haplotypes. Other than HLA genes that are associated with MS, like a deletion mutation in the CCR5 chemokine receptor gene. Further, there is the locus on chromosome 19q22 near the apolipoprotein C1 and the gene encoding the interleukin 7 receptor alpha chains
Resume
3
(IL7R) is considered as a significant risk factor for multiple sclerosis.
The infectious etiology of MS is been described. Some viruses and microbs that are implicated with the pathogenesis of the disease are: humans- JC papilloma virus, the human T-cell lymphotropic or leukemia virus type I (HTLV-I), brucella (neurobrucellosis), Measles, Varicella, Herpes simplex, respiratory syncytial virus, Inue-Melnick virus, LM7, JMH-virus, “carp” and bone marrow agent, vaccinia Parainfluenza 1, 2, 3, Influenza A, B, Human Herpes virus – 6, Rubella, Epstein-Barr, Mumps, Coronaviruses, Adenoviruses, HTLV-I and II, Simian virus-5, Rabies MS-associated retrovirus, scrapie-like agent, Simian chimpanzee, SMON-like virus, Cytomegalovirus, Simian virus 5 and Tick-borne flavivirus. A bacterium implicated to the genesis of MS is the Borrelia Burgorferi .
Autoimmunity in Multiple sclerosis: In MS, the loss of regulatory cells in the form of suppressor cells is met. The activity of suppressor CD8+ T cells is reduced, as well as the autologous mixed lymphocyte reactions, which seems to be an indicator of autoreactive cell suppression. Furthermore, the suggestion that an immune reaction to myelin antigens plays an important role in the immunopathogenesis of MS is supported by the isolation and characterization of a particular type of T-cells, the autoreactive T-cells from the blood and the CSF of MS patients. The breakdown of the blood brain barrier (BBB)
Resume
4
may affect the self-tolerance, because it gives to the CNS-reactive lymphocytes an easy access to the normally inaccessible antigens. Alternatively, a primary event such as infection or injury might release CNS antigens into the periphery, where they might activate corresponding autoreactive cells. However, this wasn’t enough to explain the MS immunopathology. Thus, a prime autoantigen that elicits the autoimmune response in MS has to be implicated. Finally, the upregulation of the costimulatory molecules may be implicated in the pathogenesis of MS. A study about MS plaques and inflammatory stroke lesions from the same brain showed that even if B7.2 was expressed in both lesions, the expression of B7.1 was restricted to MS plaques. The enhanced expression of B7.1 seems to collate with the activity of the disease. Additionally, The increased levels of PLP-reactive T-cells in the blood of MS patients compared with controls were also reported; similarly, PLP is a potent inducer of EAE in the experimental animals.
Resume
5
Therapies applied on MS patients
There is no specific treatment for MS. The treatment is directed toward controlling the symptoms, the acute relapses and preventing or delaying the exacerbations and the complications.
When we distinguish whether the patient experience a new relapse or it is a “pseudoexacerbation, corticosteroidal therapy is indicated. Corticosteroids are used during the last 35 years on MS patients. They provide a short-term clinical benefit by reducing the severity and shortening the duration of the attacks by 1 to 2 weeks. The onset of the improvement starts within three days and sometimes within few hours. The immunosuppressive and anti-inflammatory effects of steroids coexist. Methylprednisolone affects the inflammatory response in order to reduce the edema and improve the nerve conduction for speeding the recovery and to reconstruct the blood–brain barrier. In high concentrations, steroids suppress all phases of inflammation like exudation, proliferation and scar formation. As a result, there is a reduced secretion of vasoactive and chemoactive factors, a diminish release of lipolytic and proteolytic enzymes, decreased extravasations of leukocytes to the areas of the injury and reduced fibrosis. Also they inhibit the expression of endotoxins and proinflammatory cytokines, like COX-2 and NOS2.
Resume
6
The immunological mechanisms of methylprednisolone include the induction of unselective immunosupression, the inhibition of Th1 cytokine secretion, the reduction of CD4 cell levels, as well as the inhibition of MHC class II molecules expression. Additionally, lymphocytopenia is caused, as well as reduction of the expression of adhesion molecules and also blockage of the chemotactic cytokines. Corticosteroids have been shown to decrease IgG synthesis in the CNS and to reduce the CSF antibodies to MBP and OCBs Studies provided evidence that methylprednisolone suppresses the expression of genes associated with T-cell differentiation and activation, which may contribute to its beneficial effect in relapses of MS. Thus, the effects of MP on the membrane-bound and intracellular receptors causes the downregulation of growth factor and proinflammatory cytokine gene expression by inhibiting transcription through the DNA binding locus of the glucocorticoid receptors. Some of these genes are identified to be: the pro-opiomelanocortin and genes for COX-2, NOS2, and inflammatory cytokines. These genes may downregulate the HPA-axis. In the acute relapse, 500-1000mg of IV methylprednisolone in 5% dextrose solution is usually administered for 5 to 10 days, over 1-2 hours. A typical tapering regimen follows the termination of therapy. It must be mentioned that before the onset of steroidal treatment, infections should be excluded and the administration of glucocorticosteroids should be induced

Resume
7
in the morning, in order to diminish the HPA-suppression. The side effects of the corticosteroidal treatment seem to be minimal and transitory. These side effects include mental changes, confusion, depression, insomnia, fluid retention, weight gain, acne, gastric disturbances. The interferons are anti-inflammatory cytokines and they present antiviral, antineoplastic and immunomodulatory activity. Interferons are classified according to the cell type from which they were initially delivered, into two basic types. Type I IFNs (α and β) and Type II IFNs. IFNßβ was the first drug that could modify the course of MS. In this disease, two forms of IFNß are used: the IFNβ -1a and IFNβ -1b. The IFNβ -1a (Avonex and Rebif) is a glycosylated interferon, chemically unaltered and it is produced in Chinese hamster ovary cell line. IFNβ-1b (Betaferon) is chemically modified form from the naturally acquiring human beta-interferon. It is also genetically engineered, produced in Escherichia Coli cell lines. It is not glycosylated . The exact mechanism of IFNβ action in MS treatment is still unclear. However, there are several potential immunological effects of the IFNβ administration. IFNβ inhibits the mitogen-induced proliferation of T-cells as well as the expression of cell activation markers that contributes to the formation of MS plaques. Furthermore, it was demonstrated that the IFNβ inhibits the release of IFNγ from the activated T-cells.
Resume
8
Additionally, IFNβ downregulates the MHC class II expression on APCs and costimulatory molecules B7/CD28 and CD40:CD40L, and possibly reduces the APCs within the CNS. Other scientists demonstrated that IFNβ reduces the migration of cells across the BBB by an effect on adhesion molecules and matrix metalloproteinases. IFNβ could downregulate the IFNγ induced class II molecule expression. IFNβ reduces the secretion of MMP-2 and MMP-9 that depend on the IL-2. IFNβ may act therapeutically by the downregulation of IL-2 cell surface receptor expression and by the reduction of the IL-2 affinity for the T-cell surface The IFNβ also inhibits the activation of microglia with the reduction of TNF-a and IL-1. Additionally, they induce the reduction of the expression of the inegrin very late VLA-4 on the mononuclear cells and also increases the intracellular and CSF of anti-inflammatory cytokines, such as IL-10. IFNβ triggers the expression of Th2 cytokines. It was shown IFNβ upregualtes IL-10 mRNA expression and serum IL-10 levers increase. Furthermore, the increased expression of growth factor-β and of Th2 cytokine IL-6 and K-2 are also documented. The expression of IL-6 is associated with the immunoregulatory benefits, but it also seems to cause the flu-like syndrome as a major side effect of IFNβ therapy. Also interferons cause the reduction of Th1 cytokines like IL-12, TNF-a and IFNγ and decrease the ratio of IL-12/IL-10. IFNβ also inhibits the production of inducible nitric oxide synthase (iNOS), which generates the nitric
Resume
9
oxide (NO) that damages myelin and oligodendrocytes. IFNβ stimulates the murine astrocytes to produce Nerve Growth Factor up to 40 times than of normal levels and subsequently to protect the axons. Treatment with IFNβ enhances the pro-apoptotic and suppresses the anti-apoptotic cellular components. The adverse effects of IFNß administration are many. The most frequent side effect is the flue like syndrome that occurs in 50% of the treated patients. The flu-like syndrome, as mentioned earlier, may be related to the production of IFNγ, TNF-a and IL-6. IFNß administration also produces reactions at the injection sites, in 90% of patients, like pain, redness, induration or rarely, skin necrosis. Other side effects include dizziness, agitation, insomnia and anxiety, depression, myelosupression, gastrointestinal symptoms. Most of the patients that receive IFNß will develop antibodies to this molecule. These antibodies are of two types: the binding antibodies (BAbs) and the neutralizing antibodies. Nabs could affect negatively the biological activity of IFNß and weaken the therapy. Some studies suggested that the presence of Nabs is correlated with the expression of certain genes. Higher doses of Betaseron and Rebif present increased risk of developing Nabs (30-40% and 15-25% respectively), than Avonex (2-10%). to the restoration of the defective immune regulation. Several experimental studies tried to demonstrate the activity if GA on neuroprotection process. However, the
Resume
10
protection in one anatomical region of the nervous system may be followed by damage elsewhere
Glatiramer acetate (GA) is also used in the immunomidulation of the disease. It is a synthetic mixture of random acetate salts of polypeptides, similar to MBP which are composed of four naturally occurring amino acids, L-alanine, L-glutamic acid, L-lysine, and L-tyrosine. It was synthesized, in order to be used in the investigation of the interaction of myelin proteins and lipids that seem to induce EAE, but In contrary, it was found that the animals were protected. There are several proposed mechanisms of the action of glatiramer acetate in the treatment of MS. 1) Competitive binding to molecules of the MHC complex in preference to myelin protein antigens: glatiramer acetate has at least a partial cross-reactivity with MBP. It reacts with monoclonal antibodies that are directed against MBP and with T-cell or T-cell lines, which are sensitized to MBP. Furthermore, the binding of the glatiramer acetate to MHC class II molecules on the antigen presenting cells (APCs) may associates with the antigen presentation of T-cells. Additionally, GA can inhibit binding of PLP and MOG to MHC molecules on antigen-presenting cells. Other studies demonstrated a direct ‘‘promiscuous’’ binding of GA to human antigen-presenting cells and HLA-DR molecules. In addition, GA can inhibit binding of MBP or the MBP peptide p84–102 to these cells through competition for MHC class II sites. 2) Immune Deviation from Th1 to Th2 Phenotype: Due to the fact
Resume
11
that GA functions as an antigen, it can induce proliferation of T-cells from controls and MS patients, and GA reactive T-cell lines, which secrete cytokines with a Th2 anti-inflammatory profile. Hafler and colleagues confirmed these findings and characterized GA as a ‘‘universal antigen’’.it was documented that the GA-reactive lymphocytes had a significant Th2 bias, in comparison with MBP-reactive cells.The MS patients who were treated with GA do not differ in their T-cell expression of IFN-γ, compared with untreated patients. Chen and colleagues demonstrated that the Th2-biased response with GA is sustained over long-term treatment. Also it was found that the long-term administration decreased the precursor frequency of GA-reactive T-cells. However, the sustained response to GA remained Th2-biased and partially cross-reactive with MBP and MBP peptide. 3) Preferred binding of GA MHC complexes over MBP-MHC complexes to appropriate T-cell receptors (TCR) and Bystander Suppression: GA stimulates the GA-reactive T-cells, which present with Th2 properties. The GA-reactive, Th2-polirized T-cell phenotype seems to recognize myelin antigens in a non-specific way and mediate bystander suppression. GA-reactive Th2 cells secrete suppressor cytokines and decrease inflammation by inducing bystander suppression. As GA is metabolized, the antigens that are presented within the CNS cannot be GA, and must originate endogenously. It is hypothesized that the myelin damage products that are presented by APCs
Resume
12
again stimulate the GA-specific Th2 cells. Furthermore, the migration of T-cells from MS patients under GA treatment was decreased in comparison with T-cells from untreated patients. Prat and colleagues documented that IFN-β inhibited Th1 cells, while GA enhanced the migration of Th2 cells, by comparing Th1 and Th2 lymphocytes migration into the BBB. 4) Induction of tolerance in MBP-specific T-cell:As the therapy continues, GA-specific T-cells decrease. For this decrease, induction of anergy or apoptotic cell death was suggested as potential mechanisms of action. Studies suggested that GA may act differently in CD4 and CD8 cells, but these two cell populations cooperate in order to change the immunological processes in MS. It must be mentioned that the MBP-specific T-suppressor cells may keep some Th1 properties or they may shift back to Th1 profile when they are reactivated in vivo, suggesting that GA-specific Th2 cells appear to be confined to their suppressor profile. 5) Restoration of defective immune regulation:GA may influence the CD8 T-cells, which are reduced in MS patients. Administration of GA can regulate the CD8 response and increase their levels in normal values. It is obvious that these events lead to the restoration of the defective immune regulation. Several experimental studies tried to demonstrate the activity if GA on neuroprotection process. However, the protection in one anatomical region of the nervous system may be followed by damage elsewhere.
Resume
13
The III trial first studies presented a 33% reduction in relapses and it was shown that GA-treated patients tented to improve or remained stable. The side effects of GA are minimal and it is generally well tolerated. The primary side effect is the local injection site reactions that occur in 90% of patients. They consist of erythema with or without induration.
Antigenic antibodies are also immunomodulator agents for MS. Studies were conducted by these observations on the a-4 integrin antagonists and more precisely on the monoclonal antibody natalizumab. Its mechanism of action is expressed as a selective inhibition of adhesion and consequently blocks the integrin-mediated leukocyte migration. Natalizumab binds to a-4 integrin that is expressed on the surface of activated lymphocytes and monocytes. The interaction of a-4β1 inegrin with VCAM-1 is critical for all T-cell migration, except of neutrophils, into CNS. VCAM-1 is expressed at high levels in the blood vessels in the CNS during MS exacerbations. Thus, by blocking this interaction, the inhibition of exacerbations could hypothetically achieve. Krumbholz and colleagues demonstrated that natalizumab disproportionately increases the circulating pre-B and B-cells in MS. More precisely, it was shown that natalizumab therapy increased CD19+ mature B cells more than other lymphocytes or monocytes in the blood. The increase of immature CD19+CD10+ pre-B was more significant. These events were stable during a 16-month treatment. Additionally, the levels of transcripts of the
Resume
14
lymphocyte precursors Vpreβ1 and DNTT were increased more than transcripts for CD34. This observation suggests that the effects and side effects of natalizumab are partially mediated by actions on B-cells. In a placebo-controlled trial (AFFIRM), relapsing-remitting patients appeared to present with less inflammatory brain lesions and fewer relapses over 6 months. More precisely, it was observed a 66% reduction of relapses, while 76% of patients were relapse free. Gd-enhancing lesions were decreased by 92% and the number or T2 lesion was reduced by 80%. No clinical and MRI activity was presented in 46% of natalizumab-treated patients and 14% in placebo group. However, natlizumad was implicated with the appearance of PML (progressive multifocal leukoencephalopathy) and it was withdrawn from the market for several years. However the risk of developing PML was almost 1%. Other side effects include headache, nausea, urticaria and rigors. FTY720 (fingolimod) is an immunomodulatory that seems to be effective in patients with relapsing MS. It has several mechanism of action. FTY720 is a structural analogue of sphingosine, an endogenous lysophospholipid, which antagonizes the sphingosine-1-phosphate receptors (S1P1) after biotransformation to FTY720-phosphate on both T- and B-cells. Consequently, it traps the S1P/S1P1-dependent lymphocytes in secondary lymphoid organs, reducing their availability for cell-mediated immune responses. More precisely, Mehling and colleagues demonstrated
Resume
15
that treatment with FTY720 reduces naïve T cells and central memory T cells, but not effector memory T cells, in blood, without affecting T cell function. This is presumably because naïve T-cells and TCM express the homing receptor CCR7, allowing recirculation to secondary lymphoid tissues on a regular basis and, thus, trapping of the cells by FTY720 in lymph nodes. Other observations suggest that FTY720 also enhances the direct actions on glial and precursor cells of the CNS, which may be relevant for the neural repair after injury. FTY720 was synthetically developed from an immunosuppressive natural product, the ISP-1 (myriocin) that is isolated from the culture of the vegetative fungus Isaria sinclairii. The first observations for the drug were obtained from clinical trials in renal transplantation. In FREEDOMS study (phase III), there was a 55% decrease in annual relapse rate at 2 years with fingolimod at 0.5 mg, compared to placebo. Also the risk of progression in EDSS score was reduced by 30% over the 2-year study period in patients receiving fingolimode than in placebo group (p = 0.02). Significantly fewer new or enlarged lesions on T2-weighted images were seen. Mitoxantrone is an antineoplastic agent. The beneficial effects of Mitoxantrone on MS were provided by several studies. It was reported that mitoxandrone was more effective in relapsing-remitting and primary progressive MS patients. There are several, potential mechanisms of mitoxantrone action. This agent seems to have cytotoxic, immunosuppressive, antiviral and
Resume
16
antibiotic effect. Possibly, mitoxantrone acts on both DNA and RNA synthesis, but most studies demonstrated that it interferes with DNA synthesis and repair. Mitoxantrone targets the proliferating immune cells like macrophages, B- and T-lymphocytes. Mitoxantrone also decreases the CD4/CD8 ratio. Mitoxantrone affects helper and suppressor T-cells. By inhibiting T-helper activity, the drug also enhances the T-suppressor activity in vitro mitoxantrone may induce apoptosis of APCs and B-lymphocytes Also, it provided evidence of a decline in secretion of the proinflammatory cytokines IFN-γ, TNF-a and IL-2. Mitoxantrone is highly cardiotoxic agent. In order to minimize the risk of cardiotoxicity, pulses of reduced doses of mitoxantrone or the combination of mitoxantrone with dexrazoxane, which is a cardioprotective substance, are administered. Mitoxandrone also, may induce acute leukemia. The most frequent side effects include nausea, alopecia, menstrual disorder, upper respiratory tract infection and urinary tract infection. Cyclophosphamide is an alkalyating agent, due to its capability to intercalate into the DNA helix and thus it reacts with replicating DNA. It used as treatment in malignancies and in several autoimmune diseases. Cyclophosamide’s desired actions as well as the adverse effects are caused by DNA cross-linking. It affects the immune system by decreasing T-cell counts, B-cell numbers, and it induces the shift from Th1 to Th2
Resume
17
cytokine secretion. Additionally, it is known that cyclophosphamide enters the nervous system. Moreover, it reduces the CSF MBP and the intrathecally produced IgG. Cyclophosphamide is a controversial form of therapy and it has been used for more than 25 years for progressive subtypes of MS. Zephir and colleagues demonstrated that this agent might stabilize the course of the disease. Perini and colleagues reported a significant reduction of T2 lesions and Gd-enhancing lesions in SPMS patients. Cyclosporine is a cyclical undecapeptide with immunosuppressive effects. It is used in organ transplantation. Cyclosporine acts on the immune system by various ways. Its effects are mediated by its interaction with cyclophilin. Cyclosporine modifies the lymphokine gene transcription, including the downregulation of IL-2 expression, as well as IL-1, IL-3, the migration inhibitor factors and IFNγ. It also inhibits the mitogen-driven proliferative responses of T-cells; it inhibits the T-helper cells. It also enhances the production of prostaglandins by monocytes.
Methotrexate is a folic acid analogue and a widely used as an immunomodulatory agent. It may delay the progression of MS, mainly by an unselective immunosupression and reduction of T-cell counts.
Total lymphoid irradiation (TLI) may affect the progression of MS through its immunosuppressive effects. TLI procedure is done with a dose of 1980cGy in 11 fractions of 180cGy each.
Resume
18
Cladribine is the nucleoside 2-chlorodeoxyadenosine. It is considered a potent immunosuppressive agent. In MS it seems to improve the disability score, and stabilize the number of MRI lesions. The adverse events that were reported included herpes zoster, fatal hepatitis and persistently decreased levels of CD4 cell counts, bone marrow suppression.
Azathioprine is a purine analogue that inhibits both the antibody production and the cellular immune response. Thus, it affects among others the DNA and RNA synthesis. There are studies in relapsing-remitting and chronic progressive MS for the efficacy of azathioprine. It was shown the efficacy of the drug, in comparison to placebo. Another meta-analysis of seven trials documented only a small difference after 2 years in favor of azathioprine. However, the decrease in the EDSS score was not important (-0.22).
Intravenous immunoglobulins have immunomodulatory properties and are used in MS treatment. Their mechanism of action may be related to the antiidiotypic effects and suppression of the tumor necrosis factor a (TNF-a). Also, Immunoglobulins bind complement components, preventing the development of membrane-attack complex. Additionally, alterations in both CD8 and CD4 T-cells by IVIgs have been demonstrated. Immunoglobulin preparations contain antibodies against IL-1, IL-6, and the type I and II of interferons, as well as traces of anti-inflammatory cytokines such as TGF-β. Studies provided evidence of
Resume
19
fewer relapses and a trend to relapse-free periods in MS patients. Further, it was demonstrated that treatment with IVIg for the first year after the first attack that was suggestive for MS significantly decreased the incidence of a second attack. It was also shown that these patients had reduced MRI activity.
Worldwide, more than 500 patients have been treated with by autologous haematopoietic stem-cell. Although occasional relapses have been documented, MS patients that have proceeded to hematopoietic stem cell transplantation for a malignancy, presented remissions that lasted for significant time. Improvement was observed in 81% of the transplanted MS patients, by at least 1 point on the EDSS score and 24% of the patients developed relapses. After 37 months approximately, no patients did progressed and 16 were relapse-free. Follow-up studies between 9-40 months after transplantation show that 40% of patients have progressed.
Plasma exchange has a moderate effect in acute relapses in MS patients, when it was combined with ACTH or cyclophosphamide, but it is not beneficial for long-term. Studies showed that 44.1% of patients had a moderate to significant improvement in neurological deficits during 42% courses of active treatment. The highest percentage of responsiveness (60%) occurred in ten patients with optic neuritis. The responses to plasma exchange are strongly associated with the histological MS subtype.
Resume
20
New therapeutic agents are under study. Temsirolimus potentially inhibits the proliferation of T-cells that are activated by IL-2.The phase II clinical trial documented 47.8% fewer new enhancing lesions. The high dose group also had 51% fewer relapses. The side effects that developed include mouth ulceration or inflammation, menstrual dysfunction, hyperlipidemia and rashes. CTLA4Ig involves the modulation of costimulatory pathways in order to regulate T cell–mediated autoimmune responses. It was demonstrated that CTLA4Ig was well-tolerated in MS patients, with mild side effects. Additionally, these patients presented with a reduction in myelin basic protein (MBP) proliferation. Fampridine-SR is a sustained-release, orally administered potassium-channel blocker that functions on the CNS, in order to enhance conduction in demyelinated axons. Goodman and colleagues provided evidence of favorable trends for walking speed. However, these effects were not significant. Fampridine is well tolerated. Daclizumab is an IL-2 receptor a-chain specific humanized monoclonal IgG1 antibody. Rose and colleagues conducted a phase II daclizumab trial; The drug was effective in reducing the number of Gd-lesions and could improve the EDSS scores in relapsing-remitting patients, who were not controlled by IFNß therapy. Teriflunomide is a dihydro-orotate dehydrogenase inhibitor, which has immunomodulatory effects,
Resume
21
including its ability to suppress EAE. The Phase II trial demonstrated that the number of active lesions was reduced. Teriflunomide-treated patients also had significantly fewer T1 enhancing lesions, as well as new or enlarging T2 lesions and new T2 lesions. Additionally, the high dose teriflunomide group had significantly reduced T2 disease burden. The drug was well tolerated. Rituximab is a human/mouse chimeric monoclonal IgG1κ antibody raised against human CD20. A phase I rituximab trial shown that the Rituximab -induced depletion of CD19 peripheral B cells was complete (99.8%) by week 2. No serious side effects were reported. Additionally, decreased number of new Gd or T2 lesions was seen until the end of the trial. Finally, a reduction in relapses was also observed over the 72 weeks compared with the year before the initiation of treatment. Ustekinumab is a monoclonal antibody against the p40 subunit of IL-12 and IL-23. A phase II, double-blind did not provide a significant reduction in the number of Gd lesions. Side effects developed in 85% of the treated patients Alemtuzumab is a humanized monoclonal IgG1κ antibody that rose against CD52. It was found a great reduction in the number of new Gd-lesions and annualized relapse rate, but 15 of 28 patients progressed in the EDSS score during the post-treatment observation period of 18 months. The annualized relapse rate was reduced by 94% and only one patient was progressed in
Resume
22
disability. However, four cases of autoimmune thyroid disorder and one case of transient thrombocytopenia were observed Laquinimod is an oral novel immunomodulatory agent for the treatment in MS. It was provided evidence in the phase IIb study of a 40.4% reduction of the number of Gd-lesions. Laquinimod was well tolerated, with some self-limited and dose-dependent increases in liver enzymes. A case of Budd-Chiari syndrome was reported after 1 month of exposure in a patient with underlying hypercoagulability. Chaperonin 10 is a mitochondrial molecule that is involved in protein folding. Platten and colleagues conducted a phase IIa clinical trial relapse-remitting or secondary progressive MS patients. Lower levels of critical proinflammatory cytokines were observed. Additionally, a trend toward improvement in new Gd-lesions was observed, but this difference was not statistically significant. No differences in clinical outcome measures were seen. Dimethyl fumarate and its active metabolite, methyl hydrogen fumarate, for many decades it has been used in the treatment of psoriasis. It seems to decrease oxidative stress and protect axons from inflammatory mediators. Kappos and colleagues documented a decrease in the primary endpoint of mean number of Gd lesions by 69% in the 240 mg that was receiving three times daily treatment group, in comparison to placebo from week 12 to 24. The patients treated with fumarate on 240 mg
Resume
23
three times daily reduced new or enlarging T2 and T1 lesions and relapse rates by 32% compared to placebo. The side effect were higher in all fumarate groups included flushing, abdominal pain, headache, and fatigue. Primary Progressive MS Unfortunately, for primary progressive MS none of the available treatments is effective. Plenty of studies tried to observe the most effective therapeutic agent for PPMS. Among these drugs are included the following: rituximab, natalizumab, idebenone, FTY720, interferonβ-1b, sunphenon EGCG, interferonβ-1a, teriflunomide, erythropoetin , intravenous immunoglobulins and fampridine. In fact, the results for ongoing studies on this MS subtype have been disappointing with many studies to stop from phase II. On the other hand, beneficial but controversialy discussed effects were mentioned in primary progressive MS patients with predominantly spinal symptoms according to several studies with the sustained released steroid triamcinolone acetonide.
Resume
24
Personal Part
Material and Method
The main goal of this study was to observe the therapeutical effect of the immunomodulatory treatment on MS patients in relation to relapse rate, EDSS score development and progression of the disease. In this study 150 patients with either relapsing remitting MS or secondary progressive MD were included, all patients treated and observed in “Recuperation Hospital” of Iasi, during the chronic period of 2004-2011. They were divided into four groups, each of which was treated with one of the aforementioned medications. To be more exact, 38 were receiving Avonex, 41 patients were treated with Rebif, 34 with Copaxone and 37 with Betaseron. Before the initiation of treatment clinical examination, EDSS score determination and detailed medical and family history was performed, together with MRI examination, VEP, BAEP tests, clinical ophthalmologic examination, neurophycological tests and blood analyses. The medical history among other things was necessary in order to determine the precise the duration of the disease, calculated by the time of the appearance of the first symptom until the initiation of therapy was performed, as well as specification of the period between diagnosis and treatment initiation. Then, the patients were observed over months and years with minimum time of
Resume
25
observation the 9 months and maximum time the 7 years. During these years patients were under medical attention periodically. At the beginning they were followed up at three, six and nine month; then the checkup was annual, except of course of moments and conditions of need. The first nine months patients were undergoing in clinical examination and EDSS score determination, blood tests and side effects’ report. From the first year and then annually, patients were not only clinically exam and EDSS Score was estimated, but visual evoked potentials (VEPs), brainstem auditory evoked potentials (BAEPs), MRI and blood test, ophthalmologic examination and neuropgycologic tests were occurring. Of course the most important side effects were monitoring. The objective of the study is in general terms to compare the efficacy of the four used medications on MS patients and to compare the results, in order to observe which of them is better in this specific group of patients. The potency of each drug would be estimated in function with the EDSS score rate, the relapse rate and the MRI findings. Additionally, the side-effects were reported and were compared among the four different drugs. Finally, another objective of the study is to explore the psychological status of patients in function with the medication, EDSS score and relapse rates.
Resume
26
Meeting our Variables by observing our patients before the initiation of treatment The mean age of our patients at the beginning of treatment was 34,86, while 25% of them were under 27 years old and 25% were under 42,25 years old. Thus, the 75% of all patients were under 42,25 years old. The disease it is obvious in this study also that affects young population. The 62% of our patients were females and 34% MS is considered to be a “female” disease and it is documented also in this study. The 57,3% of all patients had second level educational studies and 32,0% were superiorly educated. Obviously, the 89,3% of our patients were educated, fact that points to the tendency of the disease at the educated levels. At the social status observation, the 74,0% of patients were married. Almost half of our of patients were employed (47,3%) and interestingly the 23,3% were pensioners. The last percentage is quite high, if we correlate it with the EDSS score and the age, meaning that young people with EDSS score under 3 were incapable of working. The 99.32% of patients did not have to declare any family history as regard to MS. From the 150 patients, just one woman had her mother diagnosed with MS. In 75% of all patients the diagnosis was confirmed within 4 years after the appearance of the first symptom. Also it is interested to be mentioned that in two cases the diagnosis was verified after 20 years and in 10 cases between 10 to 28 years. In
Resume
27
the last case that diagnosis was confirmed 28 years after, the first symptom appeared in childhood with sensory disturbances. On the half of our cases the initiation of therapy took place almost at the same time as diagnosis and 75% within the first 2 years after diagnosis. One patient entered the treatment 14 years after diagnosis! The 98,7% of patients were suffering from RRMS and just 1,3% of patients presented SPMS. These two SPMS patients were men! The frequency of patients under certain medications was the following: 38 of patients were treated with Avonex, 41 with Rebif, 34 with Copaxone and 37 with Betaseron. At the beginning of observations seven years ago there were only 17 patients and during the first year the total amount of patients were 50. By the end of the sixth year the patients taking part in the treatment were 143 and by the end of the seventh year they were 150. The first symptoms that ever was experienced by the patients and points to MS was pyramidal(29,5%), followed by cerebral(24,9%) and cerebellar(15,4%). Interestingly, just in the 16,1% of patients the disease appeared with visual problems. It worth to be mentioned that in two female patients the first symptom appeared after the birth of their child, showing the autoimmune nature of the disease. By the time of treatment initiation, the 78,5% of patients had presented pyramidal symptoms, which was also the predominant syndrome. Further, almost one in two patients experienced and/or cerebral/ cerebellar
Resume
28
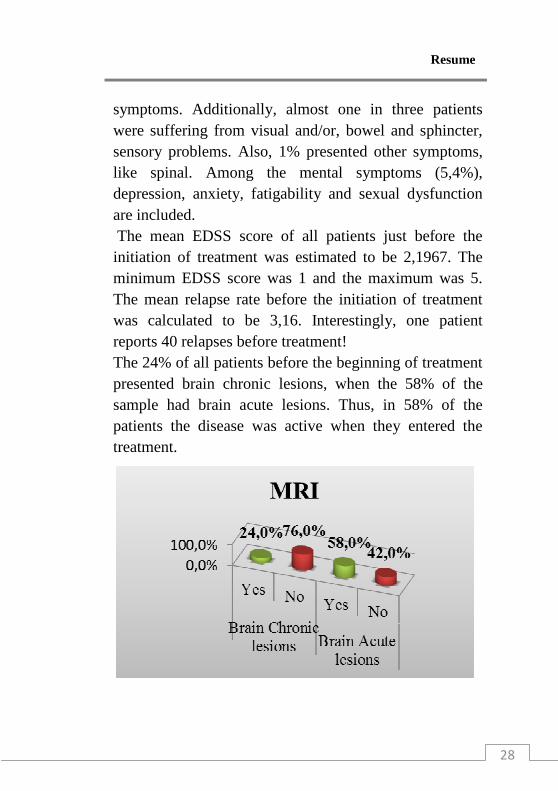
symptoms. Additionally, almost one in three patients were suffering from visual and/or, bowel and sphincter, sensory problems. Also, 1% presented other symptoms, like spinal. Among the mental symptoms (5,4%), depression, anxiety, fatigability and sexual dysfunction are included. The mean EDSS score of all patients just before the initiation of treatment was estimated to be 2,1967. The minimum EDSS score was 1 and the maximum was 5. The mean relapse rate before the initiation of treatment was calculated to be 3,16. Interestingly, one patient reports 40 relapses before treatment! The 24% of all patients before the beginning of treatment presented brain chronic lesions, when the 58% of the sample had brain acute lesions. Thus, in 58% of the patients the disease was active when they entered the treatment.
Resume
29
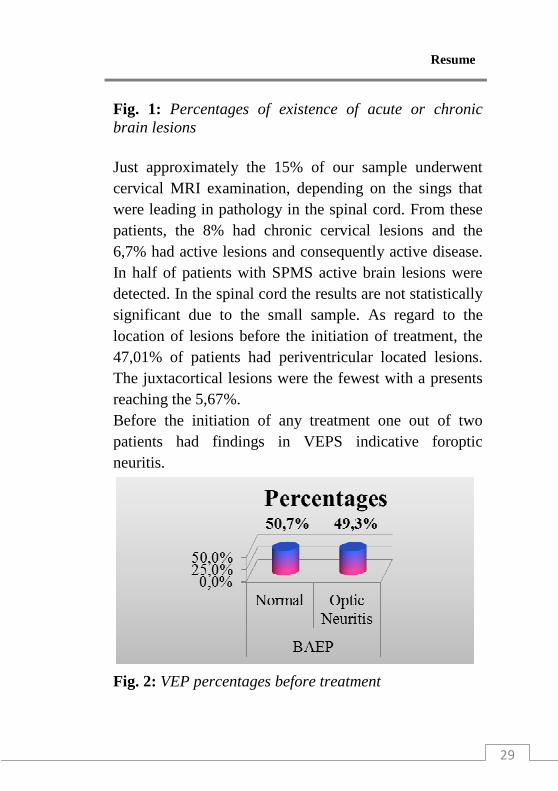
Fig. 1: Percentages of existence of acute or chronic brain lesions Just approximately the 15% of our sample underwent cervical MRI examination, depending on the sings that were leading in pathology in the spinal cord. From these patients, the 8% had chronic cervical lesions and the 6,7% had active lesions and consequently active disease. In half of patients with SPMS active brain lesions were detected. In the spinal cord the results are not statistically significant due to the small sample. As regard to the location of lesions before the initiation of treatment, the 47,01% of patients had periventricular located lesions. The juxtacortical lesions were the fewest with a presents reaching the 5,67%. Before the initiation of any treatment one out of two patients had findings in VEPS indicative foroptic neuritis.
Fig. 2: VEP percentages before treatment
Resume
30
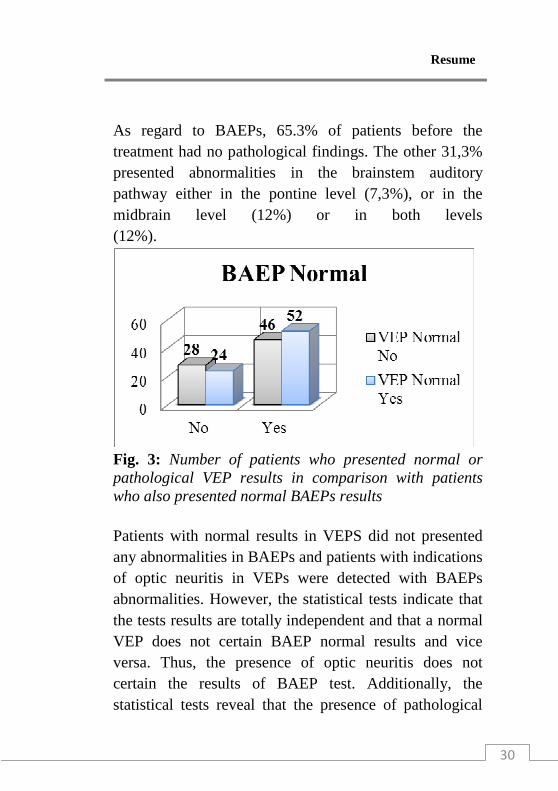
As regard to BAEPs, 65.3% of patients before the treatment had no pathological findings. The other 31,3% presented abnormalities in the brainstem auditory pathway either in the pontine level (7,3%), or in the midbrain level (12%) or in both levels (12%).
Fig. 3: Number of patients who presented normal or pathological VEP results in comparison with patients who also presented normal BAEPs results Patients with normal results in VEPS did not presented any abnormalities in BAEPs and patients with indications of optic neuritis in VEPs were detected with BAEPs abnormalities. However, the statistical tests indicate that the tests results are totally independent and that a normal VEP does not certain BAEP normal results and vice versa. Thus, the presence of optic neuritis does not certain the results of BAEP test. Additionally, the statistical tests reveal that the presence of pathological
Resume
31
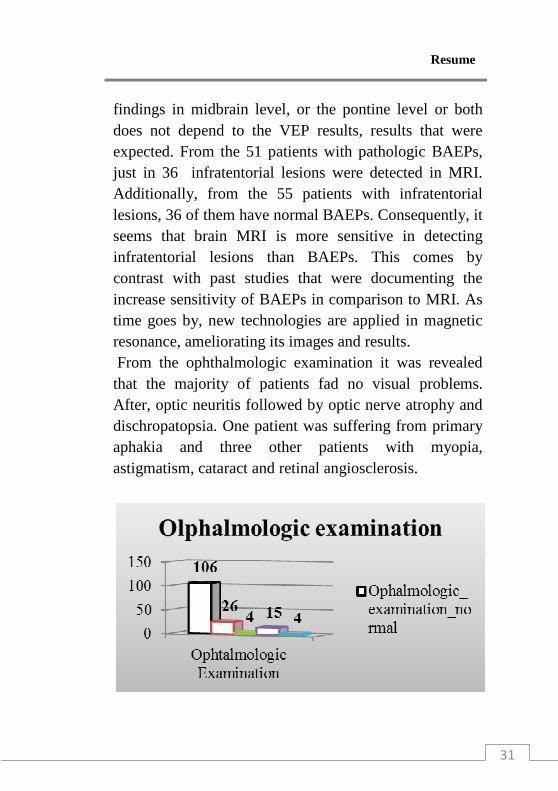
findings in midbrain level, or the pontine level or both does not depend to the VEP results, results that were expected. From the 51 patients with pathologic BAEPs, just in 36 infratentorial lesions were detected in MRI. Additionally, from the 55 patients with infratentorial lesions, 36 of them have normal BAEPs. Consequently, it seems that brain MRI is more sensitive in detecting infratentorial lesions than BAEPs. This comes by contrast with past studies that were documenting the increase sensitivity of BAEPs in comparison to MRI. As time goes by, new technologies are applied in magnetic resonance, ameliorating its images and results. From the ophthalmologic examination it was revealed that the majority of patients fad no visual problems. After, optic neuritis followed by optic nerve atrophy and dischropatopsia. One patient was suffering from primary aphakia and three other patients with myopia, astigmatism, cataract and retinal angiosclerosis.
Resume
32
Fig. 4: Ophthalmologic examination results with the number of patients
It seems that the ophthalmologic examination is no as sensitive as VEPs in detecting abnormalities pointing to optic neuritis. From the just 18 patients that had taken the HAM-A test it is demonstrated that the estimated mean value is 9.22. Thus, it seems that patients were mildly anxious just before the beginning of treatment, pointing that either the nature of the disease or the difficulties in administration and side effects of the medication did not influence their anxiety status. Additionally, the existence of lesions that could affect the biology of the brain, do not seem to interfere in this point of the study with the mood of the patient. As for the depressive status before the initiation of treatment, the mean value of HAM-D was estimated to be 10,00, meaning that most of the patients were suffering from mild depression. The maximum HAM-D value was found to be 26, which is indicative for severe depression. This score was met in a woman, in who the symptoms of the disease before the therapy included mental problems. Among all the symptoms that were observed in the period before the beginning of treatment, just the 5,4% was mental problems. However, this finding does not correlate with the mean HAM-D value that shows the domination of mild depressive feeling. One potential explanation is that patients underestimate their psychological status and cannot bring to the doctor
Resume
33
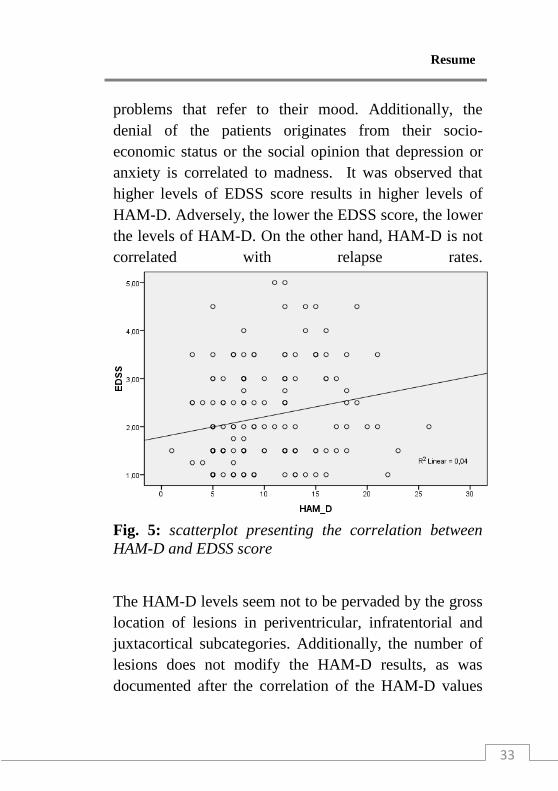
problems that refer to their mood. Additionally, the denial of the patients originates from their socio-economic status or the social opinion that depression or anxiety is correlated to madness. It was observed that higher levels of EDSS score results in higher levels of HAM-D. Adversely, the lower the EDSS score, the lower the levels of HAM-D. On the other hand, HAM-D is not correlated with relapse rates.
Fig. 5: scatterplot presenting the correlation between HAM-D and EDSS score
The HAM-D levels seem not to be pervaded by the gross location of lesions in periventricular, infratentorial and juxtacortical subcategories. Additionally, the number of lesions does not modify the HAM-D results, as was documented after the correlation of the HAM-D values
Resume
34
with the frequency of more than nine hyperintense T2 lesions. Additionally, the presence of chronic and acute lesions does not influence the HAM-D levels. However, HAM-D is related to gender, as males were observed to present higher HAM-D level than females. Social and professional status does not affect the HAM-D result. The need of changing therapy due to frequent relapses and increase in EDSS score was observed among Avonex treated patients.
Resume
35
Immunomodulation- general review
It seems that the annual relapse rate slightly increases between the fourth and fifth year of treatment in all the patients subcategories treated for more than three years. However, the annual relapse rate never exceeds the value of 0,69 that is met in the fifth year in the group of patients with five years under treatment. The deference in relapse rate between the value of the period before the initiation of treatment and the highest representative value during the seven years of observations is estimated to be 2,47. This means that every year, less than a patient will go under relapse. Until the first year of treatment the EDSS score seems to be quite stable. However, with slight fluctuations the EDSS score starts mildly increasing until the seventh year of observation that it reaches its highest value that is 2,6389. The difference of the mean EDSS score from the time before the treatment initiation and all along the seven years is calculated to be 0,4422, almost half point. The statistical significance is not important and thus, we presume that the EDSS score remains stable during the seven years with tendency of increasing. The duration of treatment does not influence the EDSS score in any administered medication of this study. The HAM-D values remain almost stable through the seven years of observation, showing permanently mild depression. None of the four different drugs did not
Resume
36
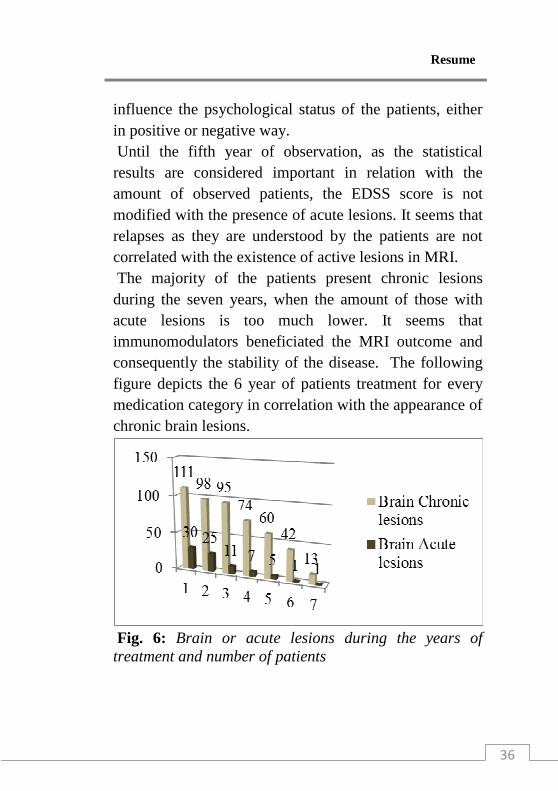
influence the psychological status of the patients, either in positive or negative way. Until the fifth year of observation, as the statistical results are considered important in relation with the amount of observed patients, the EDSS score is not modified with the presence of acute lesions. It seems that relapses as they are understood by the patients are not correlated with the existence of active lesions in MRI. The majority of the patients present chronic lesions during the seven years, when the amount of those with acute lesions is too much lower. It seems that immunomodulators beneficiated the MRI outcome and consequently the stability of the disease. The following figure depicts the 6 year of patients treatment for every medication category in correlation with the appearance of chronic brain lesions.
Fig. 6: Brain or acute lesions during the years of treatment and number of patients
Resume
37
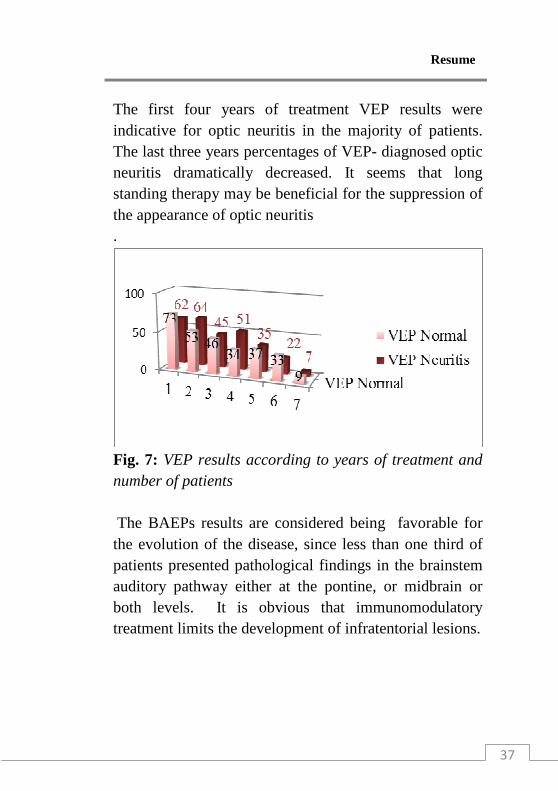
The first four years of treatment VEP results were indicative for optic neuritis in the majority of patients. The last three years percentages of VEP- diagnosed optic neuritis dramatically decreased. It seems that long standing therapy may be beneficial for the suppression of the appearance of optic neuritis .
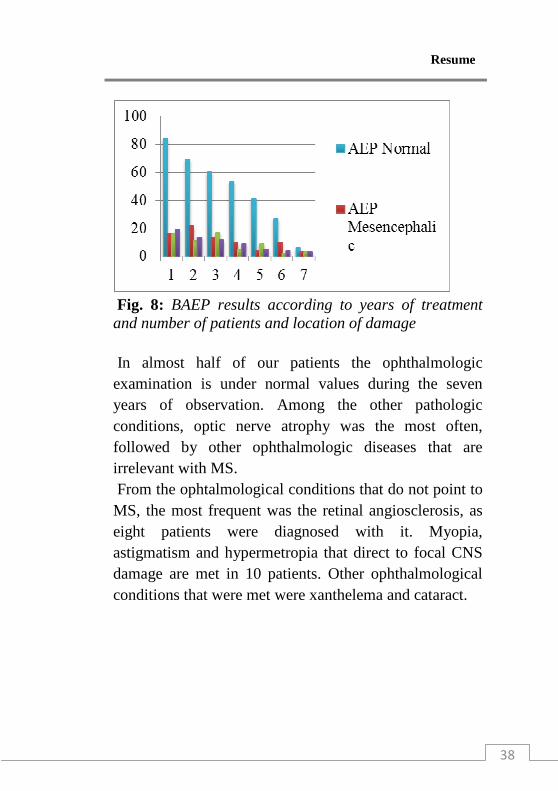
Fig. 7: VEP results according to years of treatment and number of patients The BAEPs results are considered being favorable for the evolution of the disease, since less than one third of patients presented pathological findings in the brainstem auditory pathway either at the pontine, or midbrain or both levels. It is obvious that immunomodulatory treatment limits the development of infratentorial lesions.
Resume
38
Fig. 8: BAEP results according to years of treatment and number of patients and location of damage In almost half of our patients the ophthalmologic examination is under normal values during the seven years of observation. Among the other pathologic conditions, optic nerve atrophy was the most often, followed by other ophthalmologic diseases that are irrelevant with MS. From the ophtalmological conditions that do not point to MS, the most frequent was the retinal angiosclerosis, as eight patients were diagnosed with it. Myopia, astigmatism and hypermetropia that direct to focal CNS damage are met in 10 patients. Other ophthalmological conditions that were met were xanthelema and cataract.
Resume
39
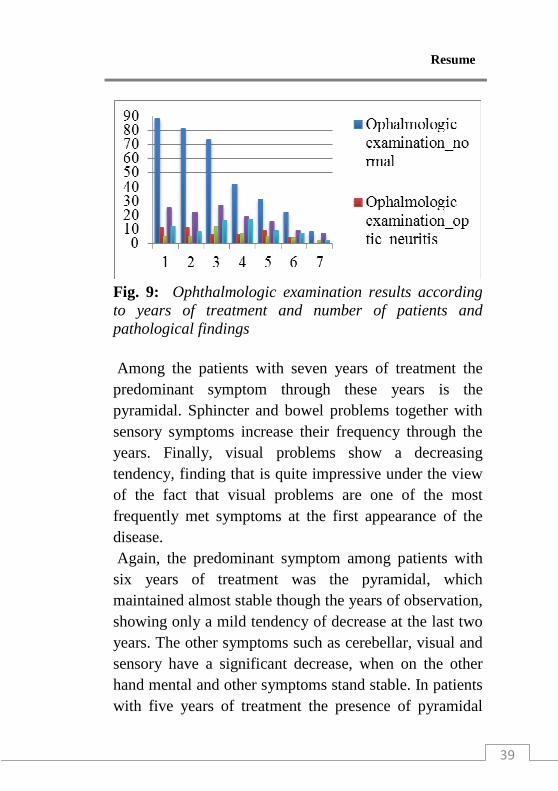
Fig. 9: Ophthalmologic examination results according to years of treatment and number of patients and pathological findings Among the patients with seven years of treatment the predominant symptom through these years is the pyramidal. Sphincter and bowel problems together with sensory symptoms increase their frequency through the years. Finally, visual problems show a decreasing tendency, finding that is quite impressive under the view of the fact that visual problems are one of the most frequently met symptoms at the first appearance of the disease. Again, the predominant symptom among patients with six years of treatment was the pyramidal, which maintained almost stable though the years of observation, showing only a mild tendency of decrease at the last two years. The other symptoms such as cerebellar, visual and sensory have a significant decrease, when on the other hand mental and other symptoms stand stable. In patients with five years of treatment the presence of pyramidal

Resume
40
syndrome is enhanced and appears much more frequently than the other symptoms, with increase tendency the first two years of treatment and decrease tendency the last year. On the other hand the cerebellar symptoms increase significantly, as well as the sphincters and bowel disturbances. Visual problems decrease in frequency together with the cerebral symptoms. The other symptoms remain quite stable.
Fig. 10: Symptoms through 7 years of treatment At the group of patients with four years of treatment the pyramidal syndrome during the whole treatment period is present. On the other hand sphincters and bowel disturbances together with mental symptoms have a significant increase. Again, the patients with three years of treatment 3 years mostly suffer from pyramidal syndrome during the whole treatment period. On the other hand sphincters and bowel symptoms have a
Resume
41
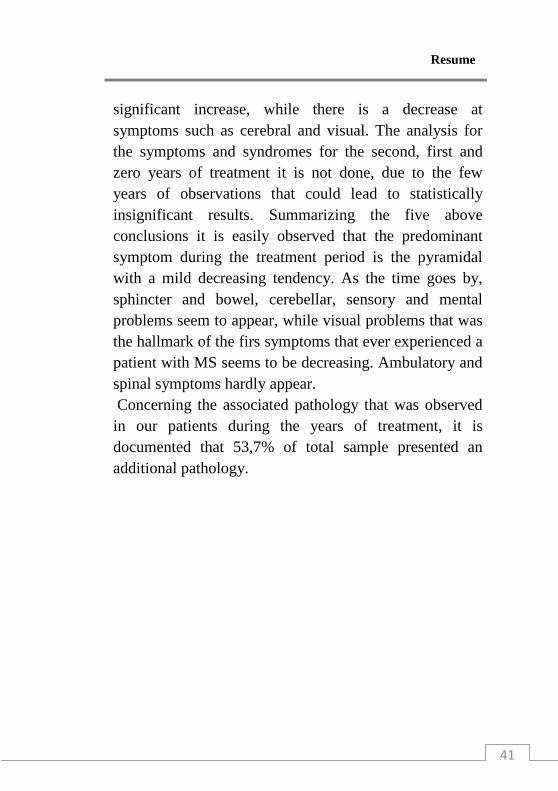
significant increase, while there is a decrease at symptoms such as cerebral and visual. The analysis for the symptoms and syndromes for the second, first and zero years of treatment it is not done, due to the few years of observations that could lead to statistically insignificant results. Summarizing the five above conclusions it is easily observed that the predominant symptom during the treatment period is the pyramidal with a mild decreasing tendency. As the time goes by, sphincter and bowel, cerebellar, sensory and mental problems seem to appear, while visual problems that was the hallmark of the firs symptoms that ever experienced a patient with MS seems to be decreasing. Ambulatory and spinal symptoms hardly appear. Concerning the associated pathology that was observed in our patients during the years of treatment, it is documented that 53,7% of total sample presented an additional pathology.
Resume
42
Fig. 11: Associated pathology in percentages The most frequent of all was dyslipidemia, which reach the percentage of 25.3%, followed by hyperglycemia (8.7%). Vertebral hernias in cervical and lumbar spinal column, associated with laminectomies or spondylofussion was found in 6% of our patients. Further, 4% of them were suffering from arachnoid cyst and iron deficiency anemia. The one of 6 patients with arachnoid cysts developed epileptic convulsions during the fourth year of treatment. However, his EDSS score or his annual relapse rate was not influenced by the
Resume
43
underlying disease. Hereditary diseases like Gilbert syndrome, Charcot Marie Tooth Neuropathy and Venus insufficiency were also recorded, as well as idiopathic diseases like Raynaud syndrome. Finally, viral and microbial infections like H1N1 infection, hepatitis B, Lyme disease and tuberculosis were among the associated pathologies of our patients. As regard to Lyme disease, patient ailed after five years of treatment. Borrelia burgdorferi is implicated in MS etiopathogenesis since it was detected in postmortem brain tissues and impressively the prevalence of MS resembles the distribution of the Lyme disease. The specific patient is worth to be mentioned that presented frequent relapses (almost every other year) and his EDSS score was estimated to be 3,5. In this point it must be mentioned that one female patient who was treated with Betaseron, was allergic to methylprednisolone and the acute relapses could not be managed. For this reason azathioprine was administered, but again she developed petechiae. This is one difficult question to answer: in case of allergy on steroids, what drug is better in the acute phase of the disease. Since now, studies have documented the beneficial and absolute effects of steroids in relapses. Another interesting point of the associated pathology analysis is the metabolic diseases. As it is already mentioned, 25.3%, of patients developed dyslipidemia and 8.7% hyperglycemia. Additionally, three patients of our set were obese and on the other hand another two women lost plenty of kilos during the first year of
Resume
44
treatment. More precisely, one Betaseron- treated patient lost ten kilos the first three months of therapy, another six the next three months and another 5 the third trimester of the observation. She was complaining for decrease appetite and the HAM-D test revealed only mild depression. Most amazing of all is that the first year of treatment she was diagnosed with dyslipidemia; her age is 39 years old! Further, another female Betaseron treated patient lost seven kilos the first trimester of observation and until the first year she had lost another ten. However, we cannot correlate a specific medication with the metabolic problems, since approximately the actual numbers of medication and dyslipidemia or hyperglycemia are the same. After detailed analysis of the EDSS score in relation to the associated pathology in each year of the treatment, it is concluded that the EDSS score is not influenced by the existence of other than MS diseases, either hereditary and idiopathic, or metabolic, neoplasias, vascular diseases and infections.
Resume
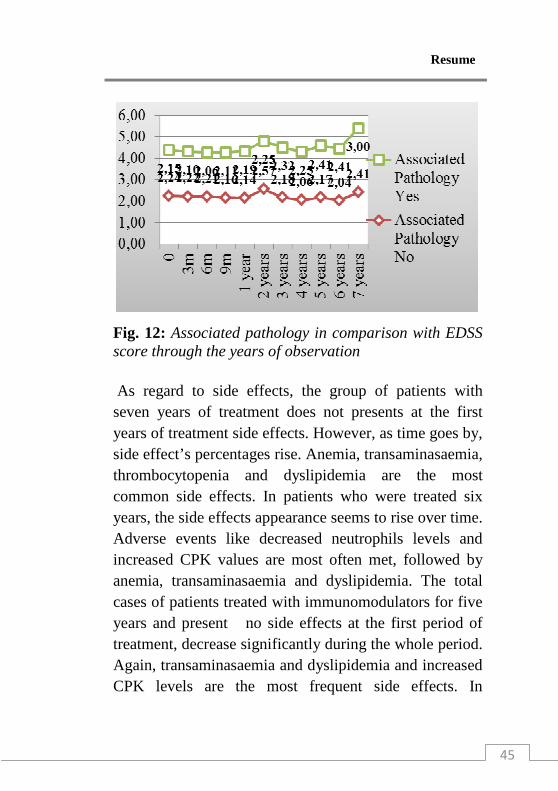
45
Fig. 12: Associated pathology in comparison with EDSS score through the years of observation As regard to side effects, the group of patients with seven years of treatment does not presents at the first years of treatment side effects. However, as time goes by, side effect’s percentages rise. Anemia, transaminasaemia, thrombocytopenia and dyslipidemia are the most common side effects. In patients who were treated six years, the side effects appearance seems to rise over time. Adverse events like decreased neutrophils levels and increased CPK values are most often met, followed by anemia, transaminasaemia and dyslipidemia. The total cases of patients treated with immunomodulators for five years and present no side effects at the first period of treatment, decrease significantly during the whole period. Again, transaminasaemia and dyslipidemia and increased CPK levels are the most frequent side effects. In
Resume
46
contrary, in patients who were under treatment for four years, the number of them with no side effects seems to increase through the respective period. Side effects like thrombocytopenia and increase levels of SGPT, SGOT and CPK have a decrease tendency from the second year of treatment and on. As regard to the side effects appeared at the patients with three years of treatment, the side effect- free number of cases seems to decrease through the years. Thrombocytopenia and transaminasaemia are the most commonly met pathological findings. However, it is estimated that in this specific group of patients the side effects remained stable. The analysis for the side effects for the second, first and zero years of treatment it is not done, due to the few years of observations that could lead to statistically insignificant results. Summarizing the results of the side effects, it seems that as time of treatment rises, the side effects- free patients decrease in actual numbers. The most frequent side effects are the thrombocytopenia, anemia, transaminasaemia, dyslipidemia, lymphocytopenia, leucocytopenia, upregulation of neutrophils with either increased or decreased values, increased CPK and LDH levels. As to anemia, it is a mild one, with no significantly decrease hemoglobin and hematocrit levels. The same is observed in transaminasaemia, while the increase in SGOT and SGPT values are 40% increase in comparison with the maximum accepted normal value. The adverse events from the treatment are not very often. Among the 150
Resume
47
treated patients, cephalalgia was met in four patients, flu-like syndrome in just two and local reaction at the injection site in one patient. The low degree of appearance of the adverse events is related with the recommendation to the patients to receive 500mg of paracetamol before and twelve hours after the administration of the medication
Resume
48
Avonex, Rebif, Betaseron and Copaxone treated- groups of patients: Special
characteristics and metanalysis In the overall set of patients, the medications are mostly applied to women. However, among them, the Betaseron treated patients were mostly males (29,41%) and the Rebif group of patients were in their majority females (30,43%); these percentages demonstrate the analogical frequencies of the patients’ gender. Betaseron was administered in younger patients (29 mean ages) and Copaxone in the oldest group in our study (39.70 years old mean age). In between there are Avonex and Rebif patients with the mean age 32.62 and 37.66 years old respectively. As for the duration of treatment for each different drug, Avonex was administered less than the other medications (of about 2 years and 7 months.
Resume
49
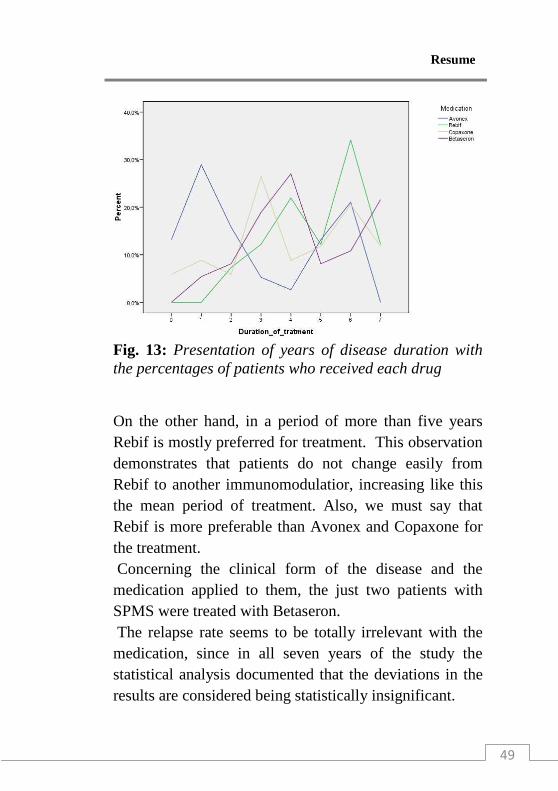
Fig. 13: Presentation of years of disease duration with the percentages of patients who received each drug
On the other hand, in a period of more than five years Rebif is mostly preferred for treatment. This observation demonstrates that patients do not change easily from Rebif to another immunomodulatior, increasing like this the mean period of treatment. Also, we must say that Rebif is more preferable than Avonex and Copaxone for the treatment. Concerning the clinical form of the disease and the medication applied to them, the just two patients with SPMS were treated with Betaseron. The relapse rate seems to be totally irrelevant with the medication, since in all seven years of the study the statistical analysis documented that the deviations in the results are considered being statistically insignificant.
Resume
50
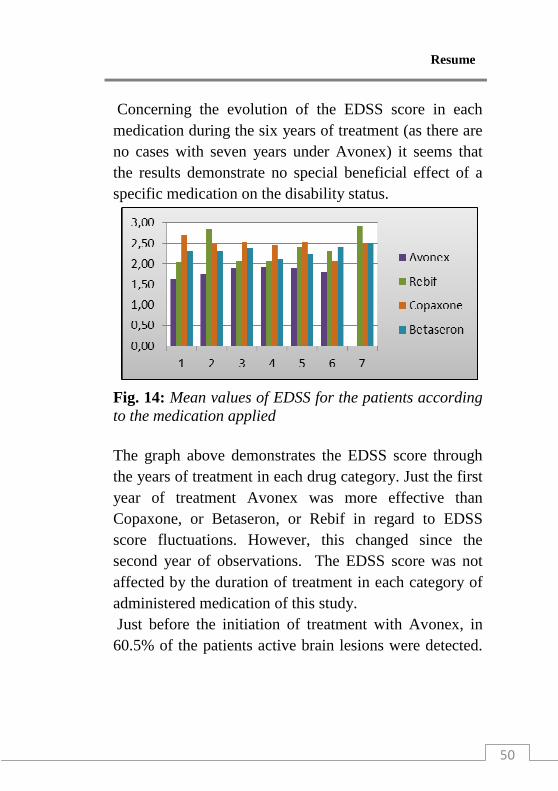
Concerning the evolution of the EDSS score in each medication during the six years of treatment (as there are no cases with seven years under Avonex) it seems that the results demonstrate no special beneficial effect of a specific medication on the disability status.
Fig. 14: Mean values of EDSS for the patients according to the medication applied The graph above demonstrates the EDSS score through the years of treatment in each drug category. Just the first year of treatment Avonex was more effective than Copaxone, or Betaseron, or Rebif in regard to EDSS score fluctuations. However, this changed since the second year of observations. The EDSS score was not affected by the duration of treatment in each category of administered medication of this study. Just before the initiation of treatment with Avonex, in 60.5% of the patients active brain lesions were detected.
Resume
51
During the six years of treatment, as there is not a sample for treatment with Avonex until seven years, most of the patients were diagnosed with chronic brain lesion. At the end of the therapy’s observation, almost all patients presented chronic brain lesions. The EDSS score in relation with the presence of either acute or chronic lesions did not seem to be influenced at the first two years of treatment with Avonex. It seems that active lesions and consequently activity of the disease does not change –at least permanently- the EDSS score. Just before the administration of treatment with Rebif, 53.7% of our patients had acute brain lesions and 22% of them had chronic brain lesions. During the seven years of treatment with Rebif the active lesions seemed to decrease dramatically their percentages and by the end of treatment observation almost all patients had chronic brain lesions. Additionally, 4.9% of the patient set under Rebif treatment presented acute cervical lesions and 9.8% had chronic cervical lesions. Again the active lesions by the end of treatment had changed into chronic state. As regard to thoracic MRI, 4.9% of Rebif-treated patients were diagnosed with thoracic active lesions just before the treatment. The EDSS score did not seemed to be influenced by the presence of active lesions at the firs years of treatment with Rebif. In the period before the initiation of treatment, 56,8% of the Betaseron patients presented acute lesions on MRI,
Resume
52
while the 35,1% had just chronic lesions. Just before the treatment with Betaseron, 8.1% of patients had cervical acute lesions and 13.5% presented chronic cervical lesions. By the end of the treatment with Betaseron in all separated groups in regard to the duration of Betaseron administration, most of the patients still had acute brain lesions. The MRI results revealed moderate improvement for the Copaxone-treated patients with mild dominance of the chronic lesions by the end of seven years observation. In Betaseron- treated patients the MRI results did not show any great improvement like the other interferon-treated patients, with the presence of active lesions in almost all patients by the end of observation period. During the first year of treatment with Betaseron the EDSS score is presents higher levels in patients with acute lesions, than in those with chronic lesions. However, the second year of treatment the EDSS score is not influenced by the presence of active lesions. The MRI that was performed before the initiation of the treatment with Copaxone revealed 61.8% acute brain lesions and 26.5% chronic brain lesions. Additionally, active cervical lesions were detected in 14.7% of patients who were treated with Copaxone, while the percentage of chronic cervical lesions was 8.8%. During the seven years of treatment with Copaxone, the patients with chronic lesions were not greatly decreased in actual numbers, with mild dominance of the chronic lesions by the end of observation. During the first two years of treatment with Copaxone, the EDSS score values
Resume
53
did not seem to be influenced by the presence of active lesions- either brain or cervical. The presence of acute or chronic lesions though the seven years of treatment is independent to the type of medication administered to the patients. It seems that MRI results are almost the same in all four drug categories, demonstrating the same favorable effect of these immunomodulators to the representational evolution of the disease by the use of MRI examination. During the first year of treatment, most patients presented normal VEP s results, irrelevant with the medication that was applied. The second year of treatment most of the patients had pathologic findings for optic neuritis in VEPs, but again this observation could not be statistically related to a specific medication. On the other hand, the third year of treatment, the Copaxone group of patients presented in their majority normal VEPs results, in contrary to the other three groups of medications. However, the deviations were statistically insignificant and the final report documented that the VEPs findings were unrelated to medications. During the following four years, most of the patients had findings pointing to optic neuritis in VEPs, with no documentation of a specific medication to influence the results either in positive or in negative way, except of the fifth year of treatment. That year it was observed that the patients who were treated with either Copaxone or Betaseron did have on the majority normal VEP results with statistically significant deviations. After all, it seems that VEPs
Resume
54
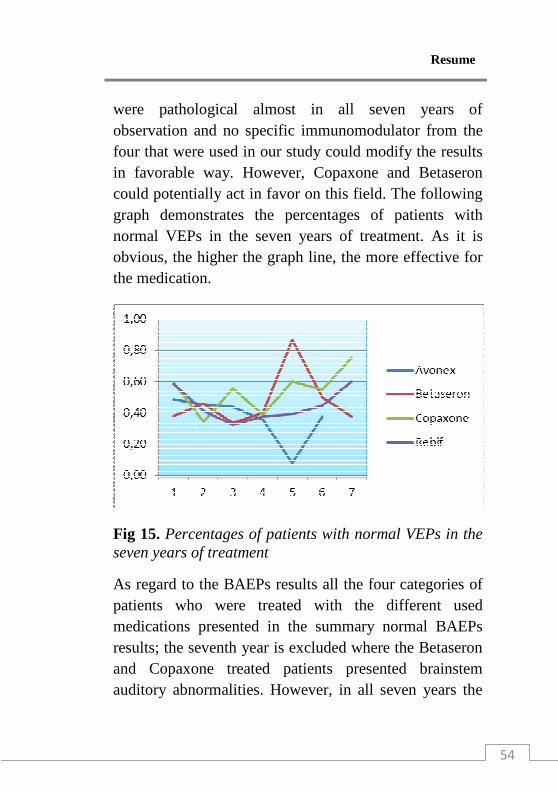
were pathological almost in all seven years of observation and no specific immunomodulator from the four that were used in our study could modify the results in favorable way. However, Copaxone and Betaseron could potentially act in favor on this field. The following graph demonstrates the percentages of patients with normal VEPs in the seven years of treatment. As it is obvious, the higher the graph line, the more effective for the medication.
Fig 15. Percentages of patients with normal VEPs in the seven years of treatment
As regard to the BAEPs results all the four categories of patients who were treated with the different used medications presented in the summary normal BAEPs results; the seventh year is excluded where the Betaseron and Copaxone treated patients presented brainstem auditory abnormalities. However, in all seven years the
Resume
55
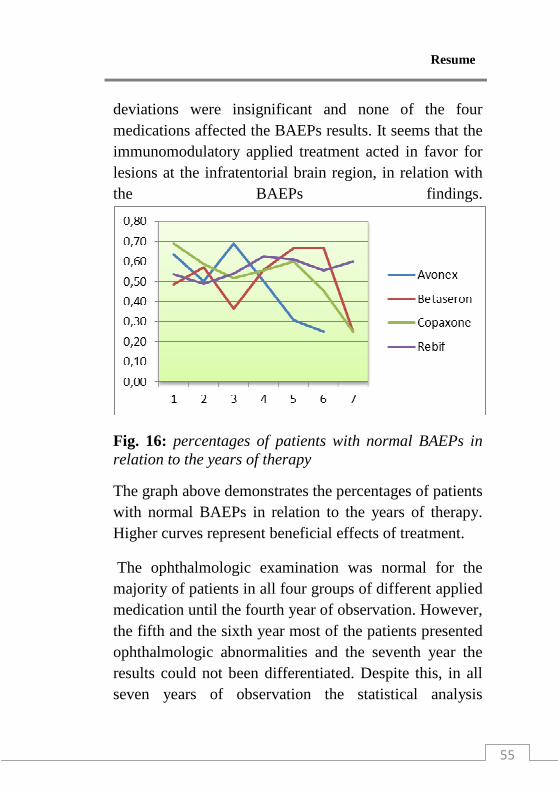
deviations were insignificant and none of the four medications affected the BAEPs results. It seems that the immunomodulatory applied treatment acted in favor for lesions at the infratentorial brain region, in relation with the BAEPs findings.
Fig. 16: percentages of patients with normal BAEPs in relation to the years of therapy
The graph above demonstrates the percentages of patients with normal BAEPs in relation to the years of therapy. Higher curves represent beneficial effects of treatment.
The ophthalmologic examination was normal for the majority of patients in all four groups of different applied medication until the fourth year of observation. However, the fifth and the sixth year most of the patients presented ophthalmologic abnormalities and the seventh year the results could not been differentiated. Despite this, in all seven years of observation the statistical analysis
Resume
56
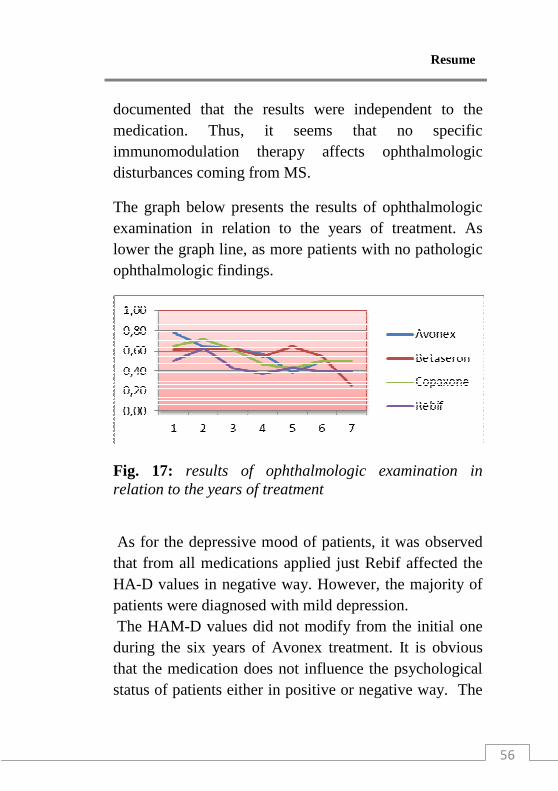
documented that the results were independent to the medication. Thus, it seems that no specific immunomodulation therapy affects ophthalmologic disturbances coming from MS.
The graph below presents the results of ophthalmologic examination in relation to the years of treatment. As lower the graph line, as more patients with no pathologic ophthalmologic findings.
Fig. 17: results of ophthalmologic examination in relation to the years of treatment
As for the depressive mood of patients, it was observed that from all medications applied just Rebif affected the HA-D values in negative way. However, the majority of patients were diagnosed with mild depression. The HAM-D values did not modify from the initial one during the six years of Avonex treatment. It is obvious that the medication does not influence the psychological status of patients either in positive or negative way. The
Resume
57
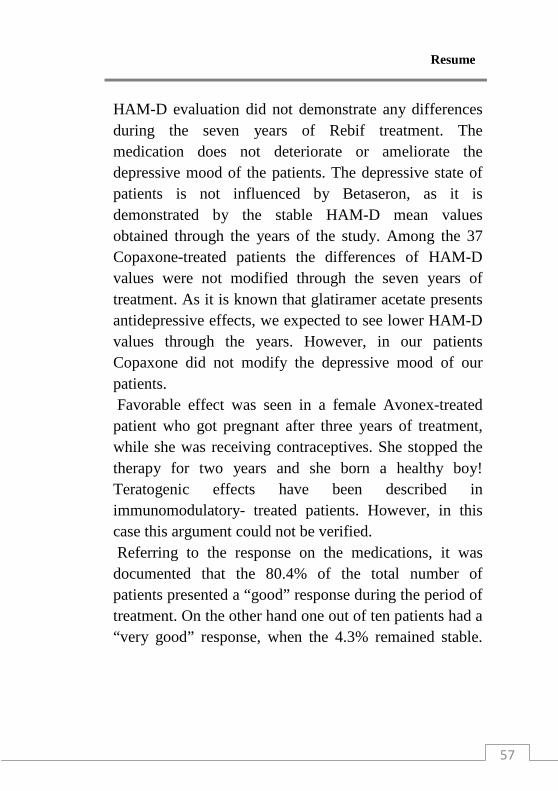
HAM-D evaluation did not demonstrate any differences during the seven years of Rebif treatment. The medication does not deteriorate or ameliorate the depressive mood of the patients. The depressive state of patients is not influenced by Betaseron, as it is demonstrated by the stable HAM-D mean values obtained through the years of the study. Among the 37 Copaxone-treated patients the differences of HAM-D values were not modified through the seven years of treatment. As it is known that glatiramer acetate presents antidepressive effects, we expected to see lower HAM-D values through the years. However, in our patients Copaxone did not modify the depressive mood of our patients. Favorable effect was seen in a female Avonex-treated patient who got pregnant after three years of treatment, while she was receiving contraceptives. She stopped the therapy for two years and she born a healthy boy! Teratogenic effects have been described in immunomodulatory- treated patients. However, in this case this argument could not be verified. Referring to the response on the medications, it was documented that the 80.4% of the total number of patients presented a “good” response during the period of treatment. On the other hand one out of ten patients had a “very good” response, when the 4.3% remained stable.
Resume
58
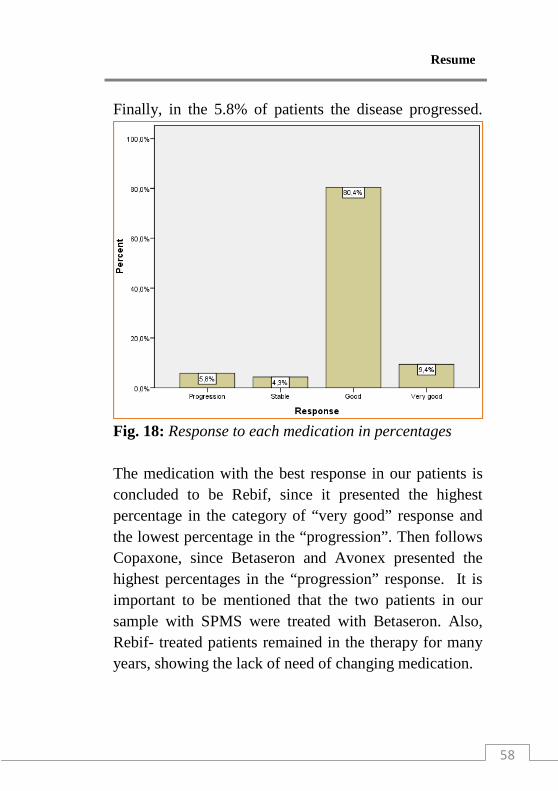
Finally, in the 5.8% of patients the disease progressed.
Fig. 18: Response to each medication in percentages The medication with the best response in our patients is concluded to be Rebif, since it presented the highest percentage in the category of “very good” response and the lowest percentage in the “progression”. Then follows Copaxone, since Betaseron and Avonex presented the highest percentages in the “progression” response. It is important to be mentioned that the two patients in our sample with SPMS were treated with Betaseron. Also, Rebif- treated patients remained in the therapy for many years, showing the lack of need of changing medication.
Resume
59
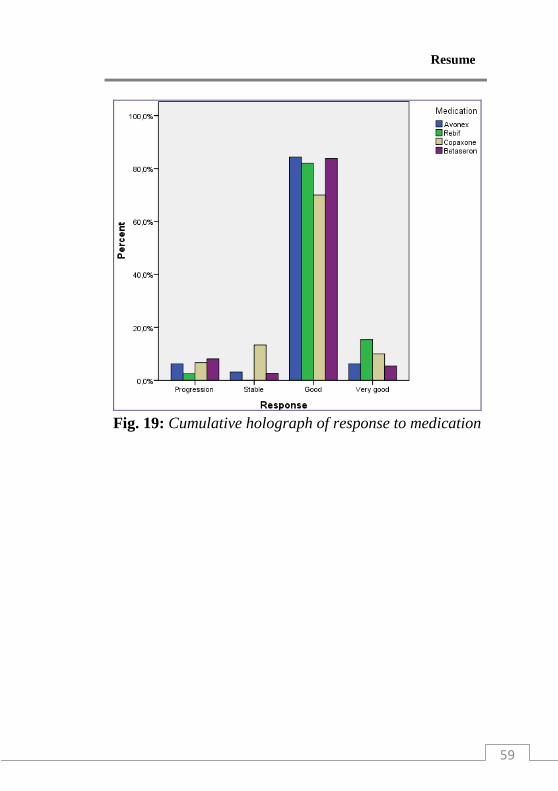
Fig. 19: Cumulative holograph of response to medication
Resume
60
Selective References
1. Airla N, Luomala M, Elovaara I, Kettunen E, Knuutila S, Lehtimäki T. Suppression of immune system genes by methylprednisolone in exacerbations of multiple sclerosis. Preliminary results. J Neurol. 2004 Oct;251(10):1215-9. 2. Alajbegovic A, Loga N, Tiro N, Alajbegovic S, Todo rovic L, Jasminika-Djelilovic. Depression in multiple sclerosis patients. Med Arh. 2011;65(2):115-8. 3. Antel Jack. Birnbaum Gary, Hans-Peter Hurtung, Angela Vincent, Clinical neuroimmunology, second edition, Oxford Academic Press 2005. 4. Applebee Angela and Hillel Panitc. Early stage and long term treatment of multiple sclerosis with interferon-β. Biologics. 2009; 3: 257–271. 5. Atkins H, Freedman M. Immunoablative therapy as a treatment aggressive multiple sclerosis. Neurol Clin. 2005 Feb;23(1):273-300, ix. 6. Banwell B., A. T. Reder, L. Krupp, S. Tenembaum, M. Eraksoy, B. Alexey, D. Pohl, M. Freedman, L. Schelensky, and I. Antonijevic. Safety and tolerability of interferon beta-1b in pediatric multiple sclerosis. Neurology, Feb 2006; 66: 472 - 476. 7. Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple
Resume
61
sclerosis. Drug Des Devel Ther. 2010 Nov 24;4:343-66. 8. Beck RW, Cleary PA, Anderson MM Jr, Keltner JL, Shults WT, Kaufman DI, Buckley EG, Corbett JJ, Kupersmith MJ, Miller NR, et al. A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. N Engl J Med. 1992 Feb 27;326(9):581-8. 9. Beck RW, Cleary PA, Trobe JD, Kaufman DI, Kupersmith MJ, Paty DW, Brown CH. The 5-year risk of MS after optic neuritis. Experience of the optic neuritis treatment trial. Optic Neuritis Study Group. Neurology. 1997 Nov;49(5):1404-13. 10. Ben-Nun A, Mendel I, Bakimer R, Fridkis-Hareli M, Teitelbaum D, Arnon R, Sela M, Kerlero de Rosbo N. The autoimmune reactivity to myelin oligodendrocyte glycoprotein (MOG) in multiple sclerosis is potentially pathogenic: effect of copolymer 1 on MOG-induced disease. J Neurol. 1996 Apr;243(4 Suppl 1):S14-22. 11. Bertolotto A. Implications of neutralising antibodies on therapeutic efficacy. J Neurol Sci. 2009 Feb 1;277 Suppl 1:S29-32. 12. Brück W, Wegner C. Insight into the mechanism of laquinimod action. J Neurol Sci. 2011 Jul 15;306(1-2):173-9. 13. Candelise Livia, Hughes Richard, Liberati Alessandro, Bernard M.J. Uitdehaag, Warlow Charles. Evidence-based Neurology: Management of
Resume
62
Neurological Disorders,. 2007, Blackwell Publishing. 14. Casadevall N., Nataf J., Viron B., Kolta A., Kiladjian J.J., Martin-Dupont P. et al. Pure red-cell aplasia and antierythropoietin antibodies in patients treated with recombinant erythropoietin. N Engl J Med 2002 346:469–475. 15. Cohen J. A., M. Rovaris, A. D. Goodman, D. Ladkani, D. Wynn, M. Filippi for the 9006 Study Group. Randomized, double-blind, dose-comparison study of glatiramer acetate in relapsing–remitting MS. Neurology, Mar 2007; 68: 939 - 944. 16. Cohen JA, Barkhof F, Comi G, Hartung HP, Khatri BO, Montalban X, Pelletier J, Capra R, Gallo P, Izquierdo G, Tiel-Wilck K, de Vera A, Jin J, Stites T, Wu S, Aradhye S, Kappos L; TRANSFORMS Study Group. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010 Feb 4;362(5):402-15. 17. Cook D. Stuart. Handbook of multiple sclerosis.. 4th ed, 2006. Taylor & Francis Group. 18. Durelli L, P Barbero, M Bergui, E Versino, M A Bassano, E Verdun, C Rivoiro, C Ferrero, E Picco, P Ripellino, et al. MRI activity and neutralising antibody as predictors of response to interferon {beta} treatment in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry, June 1, 2008; 79(6): 646 - 651.
Resume
63
19. Etemadifar M, Janghorbani M, Shaygannejad V. Comparison of Betaferon, Avonex, and Rebif in treatment of relapsing-remitting multiple sclerosis. Acta Neurol Scand. May 2006;113(5):283-287. 20. Etemadifar M, Janghorbani M, Shaygannejad V. Comparison of interferon beta products and azathioprine in the treatment of relapsing-remitting multiple sclerosis. J Neurol. Dec 2007;254(12):1723-1728. 21. Filippi M, Rovaris M, Rice GP, Sormani MP, Iannucci G, Giacomotti L, Comi G. The effect of cladribine on T(1) 'black hole' changes in progressive MS. J Neurol Sci. 2000 May 1;176(1):42-4 22. Filippini G, Brusaferri F, Sibley WA, Citterio A, Ciucci G, Midgard R, Candelise L. Corticosteroids or ACTH for acute exacerbations in multiple sclerosis. Cochrane Database Syst Rev. 2000;(4):CD001331. 23. Franciotta D, Martino G, Zardini E, Furlan R, Bergamaschi R, Andreoni L, Cosi V. Serum and CSF levels of MCP-1 and IP-10 in multiple sclerosis patients with acute and stable disease and undergoing immunomodulatory therapies. J Neuroimmunol. 2001 Apr 2;115(1-2):192-8. 24. Gilli F., P. Valentino, M. Caldano, L. Granieri, M. Capobianco, S. Malucchi, A. Sala, F. Marnetto, and A. Bertolotto. Expression and regulation of IFN /β receptor in IFNβ-treated patients with multiple sclerosis. Neurology, Dec 2008; 71: 1940 - 1947.
Resume
64
25. Goetz G. Christopher Textbook of Clinical Neurology, 3rd Edition 2007, Saunders. 26. Gregory SG, Schmidt S, Seth P, Oksenberg JR, Hart J, Prokop A, Caillier SJ, Ban M, Goris A, Barcellos LF, Lincoln R, McCauley JL, Sawcer SJ, Compston DA, Dubois B, Hauser SL, Garcia-Blanco MA, Pericak-Vance MA, Haines JL; Multiple Sclerosis Genetics Group. Interleukin 7 receptor alpha chain (IL7R) shows allelic and functional association with multiple sclerosis. Nat Genet. 2007 Sep;39(9):1083-91. 27. Hellwig Kerstin, Christian Beste, Sebastian Schimrigk and Andrew Chan. Immunomodulation and postpartum relapses in patients with multiple sclerosis. Therapeutic Advances in Neurological Disorders (2009) 2(1) 7–11. 28. Herndon M. Robert. Multiple sclerosis : immunology, pathology, and pathophysiology. Demos Medical Publishing, 2003. 29. Huang R, Hughes M, Mobley S, Lanham I, Poduslo SE. APOE genotypes in African American female multiple sclerosis patients. Neurosci Lett. 2007 Feb 27;414(1):51-6. 30. Kallaur AP, Kaimen-Maciel DR, Morimoto HK, Watanabe MA, Georgeto SM, Reiche EM. Genetic polymorphisms associated with the development and clinical course of multiple sclerosis (review). Int J Mol Med. 2011 Oct;28(4):467-79.
Resume
65
31. Kappos L., A. Traboulsee, C. Constantinescu, J. -P. Erälinna, F. Forrestal, P. Jongen, J. Pollard, M. Sandberg-Wollheim, C. Sindic, B. Stubinski, B. Uitdehaag, and D. Li. Long-term subcutaneous interferon beta-1a therapy in patients with relapsing-remitting MS. Neurology, Sep 2006; 67: 944 - 953. 32. Karandikar NJ, Crawford MP, Yan X, Ratts RB, Brenchley JM, Ambrozak DR, Lovett-Racke AE, Frohman EM, Stastny P, Douek DC, Koup RA, Racke MK. Glatiramer acetate (Copaxone) therapy induces CD8(+) T cell responses in patients with multiple sclerosis. J Clin Invest. 2002 Mar;109(5):641-9. 33. Khatri B. O., MD, S. Man, MD, PhD, G. Giovannoni, MBBCh, PhD, A. P. Koo, MD, J-C Lee, MS, B. Tucky, BSc, F. Lynn, MS, S. Jurgensen, MPH, J. Woodworth, PhD, S. Goelz, PhD, P. W. Duda, MD, PhD, M. A. Panzara, MD, MPH, R. M. Ransohoff, MD and R. J. Fox, MD, Effect of plasma exchange in accelerating natalizumab clearance and restoring leukocyte function. NEUROLOGY 2009;72:402-409 34. Khurana SR, Bamer AM, Turner AP, Wadhwani RV, Bowen JD, Leipertz SL, Haselkorn JK. The prevalence of overweight and obesity in veterans with multiple sclerosis. Am J Phys Med Rehabil. 2009 Feb;88(2):83-91. 35. Koch-Henriksen N, PS Sorensen, K Bendtzen, and EM Flachs. The clinical effect of neutralizing
Resume
66
antibodies against interferon-beta is independent of the type of interferon-beta used for patients with relapsing-remitting multiple sclerosis. Multiple Sclerosis, Mar 2009; vol. 36. Lanzillo R, Orefice G, Quarantelli M, et al: Atorvastatin combined to interferon to verify the efficacy (ACTIVE) in relapsing-remitting active multiple sclerosis patients: a longitudinal controlled trial of combination therapy. Multiple Sclerosis 2010; 16: 450–454. 37. Leussink VI, Jung S, Merschdorf U, Toyka KV, Gold R. High-dose methylprednisolone therapy in multiple sclerosis induces apoptosis in peripheral blood leukocytes. Arch Neurol. 2001 Jan;58(1):91-7. 38. Liguori M, Marrosu MG, Pugliatti M, Giuliani F, De Robertis F, Cocco E, Zimatore GB, Livrea P, Trojano M. Neurol Sci. 2000;21(4 Suppl 2):S825-9. 39. Lukas C, Bellenberg B, Hahn HK, Rexilius J, Drescher R, Hellwig K, Köster O, Schimrigk S. Benefit of repetitive intrathecal triamcinolone acetonide therapy in predominantly spinal multiple sclerosis: prediction by upper spinal cord atrophy. Ther Adv Neurol Disord. 2009 Nov;2(6):42-9. 40. Lundmark F, Duvefelt K, Hillert J. Genetic association analysis of the interleukin 7 gene (IL7) in multiple sclerosis. J Neuroimmunol. 2007 Dec;192(1-2):171-3.

Resume
67
41. Mascitelli Luca, Mark R. Goldstein. Is Intensive Cholesterol Lowering Detrimental in Multiple Sclerosis? Neuroepidemiology 2011;37:259 42. Miller D. H., D. Soon, K. T. Fernando, D. G. MacManus, G. J. Barker, T. A. Yousry, E. Fisher, P. W. O'Connor, J. T. Phillips, C. H. Polman, L. Kappos, M. Hutchinson, E. Havrdova, F. D. Lublin, G. Giovannoni, A. Wajgt, R. Rudick, F. Lynn, M. A. Panzara, A. W. Sandrock For the AFFIRM Investigators. MRI outcomes in a placebo-controlled trial of natalizumab in relapsing MS. Neurology, Apr 2007; 68: 1390 - 1401. 43. Miller DH, Molyneux PD, Barker GJ, MacManus DG, Moseley IF, Wagner K. Effect of interferon-beta1b on magnetic resonance imaging outcomes in secondary progressive multiple sclerosis: results of a European multicenter, randomized, double-blind, placebo-controlled trial. European Study Group on Interferon-beta1b in secondary progressive multiple sclerosis. Ann Neurol. 1999 Dec;46(6):850-9. 44. Miller DM, Weinstock-Guttman B, Béthoux F, Lee JC, Beck G, Block V, Durelli L, LaMantia L, Barnes D, Sellebjerg F, Rudick RA. A meta-analysis of methylprednisolone in recovery from multiple sclerosis exacerbations. Mult Scler. 2000 Aug;6(4):267-73. 45. Milo R, Kahana E. Multiple sclerosis: geoepidemiology, genetics and the environment. Autoimmun Rev. 2010 Mar;9(5):A387-94.
Resume
68
46. Minagar Alireza and Alexander J. Steven. Inflammatory Disorders of the Nervous System: Pathogenesis, Immunology, and Clinical Management, 2005 Humana Press Inc. 47. Minagara A, Murray TJ; PROOF Study Investigators. Efficacy and tolerability of intramuscular interferon beta-1a compared with subcutaneous interferon beta-1a in relapsing MS: results from PROOF. Curr Med Res Opin. 2008 Apr;24(4):1049-55. 48. Miron VE, Zehntner SP, Kuhlmann T, et al: Statin therapy inhibits remyelination in the central nervous system. Am J Pathol 2009; 174: 1880–1890. 49. Moharregh-Khiabani D, Linker RA, Gold R, Stangel M. Fumaric Acid and its esters: an emerging treatment for multiple sclerosis. Curr Neuropharmacol. 2009 Mar;7(1):60-4. 50. Montomoli C, Prokopenko I, Caria A, Ferrai R, Mander A, Seaman S, Musu L, Piras ML, Ticca AF, Murgia SB, Bernardinelli L. Multiple sclerosis recurrence risk for siblings in an isolated population of Central Sardinia, Italy. Genet Epidemiol. 2002 Mar;22(3):265-71. 51. Mostert JP, Ramsaransing GS, Heersema DJ, Heerings M, Wilczak N, De Keyser J: Serum uric acid levels and leukocyte nitric oxide production in multiple sclerosis patients outside relapses. Journal of Neurological Sciences 2005, 231:41-44.
Resume
69
52. Neuteboom R. F., A. C. J. W. Janssens, T. A. M. Siepman, I. A. Hoppenbrouwers, I. A. Ketelslegers, N. Jafari , E. A. P. Steegers, C. J. M. de Groot, R. Q. Hintzen. Pregnancy in multiple sclerosis: clinical and self-report scales. J Neurol (2012) 259:311–317. 53. Oksenberg JR, Barcellos LF, Cree BA, Baranzini SE, Bugawan TL, Khan O, Lincoln RR, Swerdlin A, Mignot E, Lin L, Goodin D, Erlich HA, Schmidt S, Thomson G, Reich DE, Pericak-Vance MA, Haines JL, Hauser SL. Mapping multiple sclerosis susceptibility to the HLA-DR locus in African Americans. Am J Hum Genet. 2004 Jan;74(1):160-7. 54. Olek J. Michael. Multiple sclerosis : etiology, diagnosis, and new treatment strategies. 2005 Humana Press. 55. Patten SB, Francis G, Metz LM, Lopez-Bresnahan M, Chang P, Curtin F. The relationship between depression and interferon beta-1a therapy in patients with multiple sclerosis. Mult Scler. 2005 Apr;11(2):175-81. 56. Patten SB, Metz LM. (SPECTRIMS Study Group): Interferon beta 1a and depression in secondary progressive MS: data from the SPECTRIMS Trial. Neurology. 2002;59:744–746. 57. Pihlaja H, Rantamäki T, Wikström J, Sumelahti ML, Laaksonen M, Ilonen J, Ruutiainen J, Pirttilä T, Elovaara I, Reunanen M, Kuokkanen S, Peltonen L, Koivisto K, Tienari PJ. Linkage disequilibrium between the MBP tetranucleotide repeat and multiple
Resume
70
sclerosis is restricted to a geographically defined subpopulation in Finland. Genes Immun. 2003 Mar;4(2):138-46. 58. Polman CH, O'Connor PW, Havrdova E, Hutchinson M, Kappos L, Miller DH, Phillips JT, Lublin FD, Giovannoni G, Wajgt A, Toal M, Lynn F, Panzara MA, Sandrock AW; AFFIRM Investigators. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006 Mar 2;354(9):899-910. 59. PRISMS Study Group and the University of British Columbia MS/MRI Analysis Group.. PRISMS-4: Long-term efficacy of interferon-beta-1a in relapsing MS. Neurology. 2001 Jun 26;56(12):1628-36. Erratum in: Neurology 2001 Sep 25;57(6):1146 60. Ramagopalan SV, Byrnes JK, Orton SM, Dyment DA, Guimond C, Yee IM, Ebers GC, Sadovnick AD. Sex ratio of multiple sclerosis and clinical phenotype. Eur J Neurol. 2010 Apr;17(4):634-7. 61. Rang, Dale, Ritter, Flower. Pharmacology, 6th edition, 2007, Elsevier Inc. 62. Rejdak K, Petzold A, Stelmasiak Z, Giovannoni G: Cerebrospinal fluid brain specific proteins in relation to nitric oxide metabolites during relapse of multiple sclerosis. Mult Scler 2008, 14:59-66. 63. Rieks M, Hoffmann V, Aktas O, Juschka M, Spitzer I, Brune N, Schimrigk S, Przuntek H, Pöhlau D. Induction of apoptosis of CD4+ T cells by
Resume
71
immunomodulatory therapy of multiple sclerosis with glatiramer acetate. Eur Neurol. 2003;50(4):200-6. 64. Robertson NP, Clayton D, Fraser M, Deans J, Compston DA. Clinical concordance in sibling pairs with multiple sclerosis. Neurology. 1996 Aug;47(2):347-52. 65. Sadovnick AD, Baird PA. The familial nature of multiple sclerosis: age-corrected empiric recurrence risks for children and siblings of patients. Neurology. 1988 Jun;38(6):990-1. 66. Schlaeger R, D'Souza M, Schindler C, Grize L, Kappos L, Fuhr P. Combined evoked potentials as markers and predictors of disability in early multiple sclerosis. Clin Neurophysiol. 2012 Feb;123(2):406-10. 67. Shapiro M Aaron.; Carolyn S. Jack; Yves Lapierre; Nathalie Arbour; Amit Bar-Or; Jack P. Antel. Potential for Interferon Beta–Induced Serum Antibodies in Multiple Sclerosis to Inhibit Endogenous Interferon-Regulated Chemokine/Cytokine Responses Within the Central Nervous System. Arch Neurol, Sep 2006; 63: 1296 - 1299. 68. Smolders I, Smets I, Maier O, vandeVen M, Steels P, Ameloot M: Simvastatin interferes with process outgrowth and branching of oligodendrocytes. J Neurosci Res 2010; 88: 3361–3375.
Resume
72
69. Sominanda A, Rot U, Suoniemi M, Deisenhammer F, Hillert J, Fogdell-Hahn A. Interferon beta preparations for the treatment of multiple sclerosis patients differ in neutralizing antibody seroprevalence and immunogenicity. Mult Scler. 2007 Mar;13(2):208-14. 70. Sorensen PS, Lycke J, Eralinna JP, et al; for the SIMCOMBIN study investigators: Simvastatin as add-on threrapy to interferon beta-1a for relapsing-remitting multiple sclerosis: a placebo-controlled randomized phase 4 study. Lancet Neurol 2011; 10: 691–701. 71. Tenembaum SN, Segura MJ. Interferon beta-1a treatment in childhood and juvenile-onset multiple sclerosis. Neurology. 2006 Aug 8;67(3):511-3. 72. van der Voort L., A Kok, A Visser, C. Oudejans, M Caldano, F Gilli, A Bertolotto, C. Polman, and J Killestein. Interferon-{beta} bioactivity measurement in multiple sclerosis: feasibility for routine clinical practice. Multiple Sclerosis, February 1, 2009; 15(2): 212 - 218. 73. Van Weyenbergh J, Wietzerbin J, Rouillard D, Barral-Netto M, Liblau R. Treatment of multiple sclerosis patients with interferon-beta primes monocyte-derived macrophages for apoptotic cell death. J Leukoc Biol. 2001 Nov;70(5):745-8. 74. Wallin MT, Page WF, Kurtzke JF. Multiple sclerosis in US veterans of the Vietnam era and later
Resume
73
military service: race, sex, and geography. Ann Neurol. 2004 Jan;55(1):65-71. 75. Yong VW. Differential mechanisms of action of interferon-beta and glatiramer aetate in MS. Neurology. 2002 Sep 24;59(6):802-8. 76. Zephir H, de Seze J, Duhamel A, Debouverie M, Hautecoeur P, Lebrun C, Malikova I, Pelletier J, Sénéchal O, Vermersch P. Treatment of progressive forms of multiple sclerosis by cyclophosphamide: a cohort study of 490 patients. J Neurol Sci. 2004 Mar 15;218(1-2):73-7. 77. Zivadinov R, Rudick RA, De Masi R, Nasuelli D, Ukmar M, Pozzi-Mucelli RS, Grop A, Cazzato G, Zorzon M. Effects of IV methylprednisolone on brain atrophy in relapsing-remitting MS. Neurology. 2001 Oct 9;57(7):1239-47.