psoriazis al scalpului - · pdf file35 * clinica 2 dermatologie, spitalul clinic colentina,...
TRANSCRIPT
35
* Clinica 2 Dermatologie, Spitalul Clinic Colentina, Bucureºti.2 Dermatology Clinic, Clinical Hospital, Bucharest.
PSORIAZIS AL SCALPULUI – PREZENTARE DE CAZ
SCALP PSORIASIS – A CASE STUDY
ELENA LIVIA SEVERIN, ALINA PÎRVU, CARMEN MARIA SÃLÃVÃSTRU, G.-S. ÞIPLICA
Bucureºti
CAZURI CLINICECLINICAL CASES
Summary
Psoriasis is a chronic inflammatory skin disease withmultisystemic implications and genetic predisposition,which affects approximately 2 % of the general population.The scalp is one of the most common sites of involvement,affecting more than half of the patients suffering ofpsoriasis. Topical treatments are the mainstay of treatmentfor scalp psoriasis, with the active ingredients and also thevehicle relevant to efficacy and compliance.
We present the case of a 51-year-old female patient whohas been referred to our clinic 6 months ago, for an eruptionconstituted by well-defined erythematous-scuamousplaques, intensely pruritic, located over the scalp, with anevolution period of 2 months. On the basis of clinicalpicture and histopathological findings the diagnosis of scalppsoriasis was established. The patient was treated withcalcipotriol and betamethasone dipropionate in a gel appliedonce daily, with the complete resolution of scalp lesions in 8 days and mainstay of the results (last control visit at 4 months).
Rezumat
Psoriazisul este o boalã inflamatorie cronicã cuimplicare multisistemicã ºi predispoziþie geneticã afectândaproximativ 2% din populaþia generalã. Scalpul este unadin cele mai frecvente localizãri ale bolii, fiind afectat la maimult de jumãtate din cazuri. Terapia localã constituie bazatratamentului psoriazisului scalpului, atât vehiculul, cât ºiagenþii activi jucând un rol important în obþinerea uneieficacitãþi ºi complianþe crescute.
Prezentãm cazul unei paciente în vârstã de 51 de ani,care s-a internat în clinica noastrã în urmã cu 6 luni pentruprezenþa unei erupþii alcãtuite din plãci eritemato-scuamoase, bine delimitate, intens pruriginoase, localizatãla nivelul scalpului, cu evoluþie de 2 luni. Pe baza criteriilorclinice ºi al aspectului histopatologic s-a stabilitdiagnosticul de psoriasis vulgar cu afectarea scalpului.Pacienta a urmat tratament cu dipropionat de beta-metazonã ºi calcipotriol sub formã de gel, o singurãaplicaþie pe zi, cu rezoluþia leziunilor de la nivelul scalpuluidin ziua a 8-a ºi menþinerea rezultatelor la controlul de 4 luni.
DermatoVenerol. (Buc.), 56: 35-42
Introducere
Psoriazisul este o boalã inflamatorie cronicãcu implicare multisistemicã ºi predispoziþiegeneticã, ce afecteazã aproximativ 2% dinpopulaþie [1], [2]. Afectarea scalpului apare în 50-80% din cazurile de psoriazis [3] ºi poate fi izolatãsau se poate asocia cu psoriazisul vulgar,eritrodermic, pustulos sau cu artropatia pso-
Introduction
Psoriasis is a chronic inflammatory skindisease with multisystemic implications andgenetic predisposition, which affects approximately2 per cent of the general population [1, 2]. Thescalp is affected in 50-80 per cent of psoriasiscases [3]; the condition can be singular orassociated with psoriasis vulgaris, erythro-

36
DermatoVenerol. (Buc.), 56: 35-42
riazicã [4]. Implicarea scalpului poate fi unicã, cuapariþia unei singure plãci psoriazice saumultiplã cu apariþia de plãci ce pot ocupa totscalpul, cu diseminare spre zona frontalã ºiretroauricular. Mai rar poate sã aparã alopeciedifuza datoritã efluviului telogen [5].
Calitatea vieþii pacienþilor este mult afectatãdatoritã faptului cã leziunile sunt foarte vizibileºi pruritul poate fi foarte intens. Tratamentullocal este de regulã dificil datoritã pãrului siscuamelor groase care reprezintã un obstacol înpãtrunderea substanþelor terapeutice active lanivelul epidermului profund ºi dermului.Aºteptãrile pacienþilor sunt foarte mari dartratamentul poate fi de lungã duratã, consumatorde timp ºi de resurse, ceea ce poate determina ocomplianþã redusã.
Terapia localã pentru psoriazisul scalpuluiinclude loþiuni, creme, geluri, spume conþinândglucocorticoizi, derivaþi de gudron, acid salicilicsau derivaþi de vitamina D. Sunt recomandate ºiºampoane cu gudron, acid salicilic, sulf, seleniu,ketoconazol sau zinc pyrithion [6]. Cortico-steroizii topici sunt recomandaþi ca prima linie detratament. Rãspunsul la tratament este rapid, darposibilitatea apariþiei reacþiilor adverse (atrofie,telangiectazii, tahifilaxie etc.) limiteazã durata deutilizare. Derivaþii de vitamina D sunt utilizaþipentru cazurile moderate ºi severe de psoriazis alscalpului. Se recomandã aplicaþii de 2 ori pe zitimp de 8 sãptãmâni. Reacþiile adverse potinclude: senzaþie de arsurã, prurit ºi xerozã [6].Recent a apãrut combinaþia dipropionat debetametazonã 0,05% ºi calcipotriol 0,005% subformã de gel lipofilic, cu formulã specialconceputã pentru utilizare la nivelul scalpului.Acest produs combinat are un debut al acþiuniirapid ºi eficacitate superioarã utilizãrii dipro-pionatului de betametazonã sau calcipotrioluluiîn monoterapie [7].
Caz clinic
O pacientã în vârstã de 51 de ani, din mediulurban, fãrã antecedente patologice personalesmnificative, a fost internatã în clinicã în urmã cu6 luni pentru prezenþa unei erupþii alcãtuite dinplãci eritemato-scuamoase, intens pruriginoase,localizate la nivelul scalpului, cu evoluþie de 2 luni. Pacienta aplicase tratamente locale anti-micotice (ºampoane cu ketoconazol 2%, cu sulfitde seleniu) fãrã a obþine ameliorarea acuzelor.
dermic, pustular or arthropathic psoriasis. Scalpinvolvement can be singular, with one singlepsoriasis plaque, or multiple, with plaquescovering the whole scalp and disseminatedtowards the frontal and retro-auricular areas.Diffuse alopecia triggered by telogen effluviumcan more seldom occur [5].
Patients’ lives can be seriously affected due tothe fact that lesions are very visible and prurituscan be highly intense. Local treatment is usuallydifficult due to the presence of hair and thicksquamas that can act as barriers, blocking thepenetration of active therapeutical substancesinto the deep layers of the epidermis and of thedermis. Patients’ expectations can be very highbut the treatment can last for a long time and istime- and resource-consuming, which can causelow compliance.
Local therapy in scalp psoriasis includeslotions, ointments, gels, creams containingglucocorticoids, tar derivatives, salicylic acid orvitamin D derivatives. Shampoos based on tar,salicylic acid, sulphur, selenium, ketoconazole orzinc pyritione are also recommended [6]. Topicalcortocoids are prime recommendations. Theresponse to treatment is quick but the possibilityof adverse reactions (atrophy, telangiectases,tachiphylaxis, etc.) reduces administration period.Vitamin D derivatives are used in moderate andsevere cases of scalp psoriasis – two applicationsper day for 8 weeks. Adverse reactions mayinclude burning sensation, pruritus and xerosis[6]. Recently, a lipophilic gel containing 0.05 percent betamethasone dipropionate and 0.005 percent calcipotriol has been especially conceived forscalp treatment. This compound product yieldsrapid results and is more efficacious thanbetamethasone dipropionate- or calcipotriol-basedmonotherapy [7].
Clinical case
A 51-year-old female patient from urbanmilieu, without a significant pathological history,was referred to our clinic 6 months ago for aneruption constituted by well-definederythematous-scuamous plaques, intenselypruritic, located over the scalp, with an evolutionperiod of 2 months. The patient had beforehandapplied local antimycotic treatment consisting of2% ketoconazole shampoo with seleniumsulphite addition, without amending hercondition.

37
DermatoVenerol. (Buc.), 56: 35-42
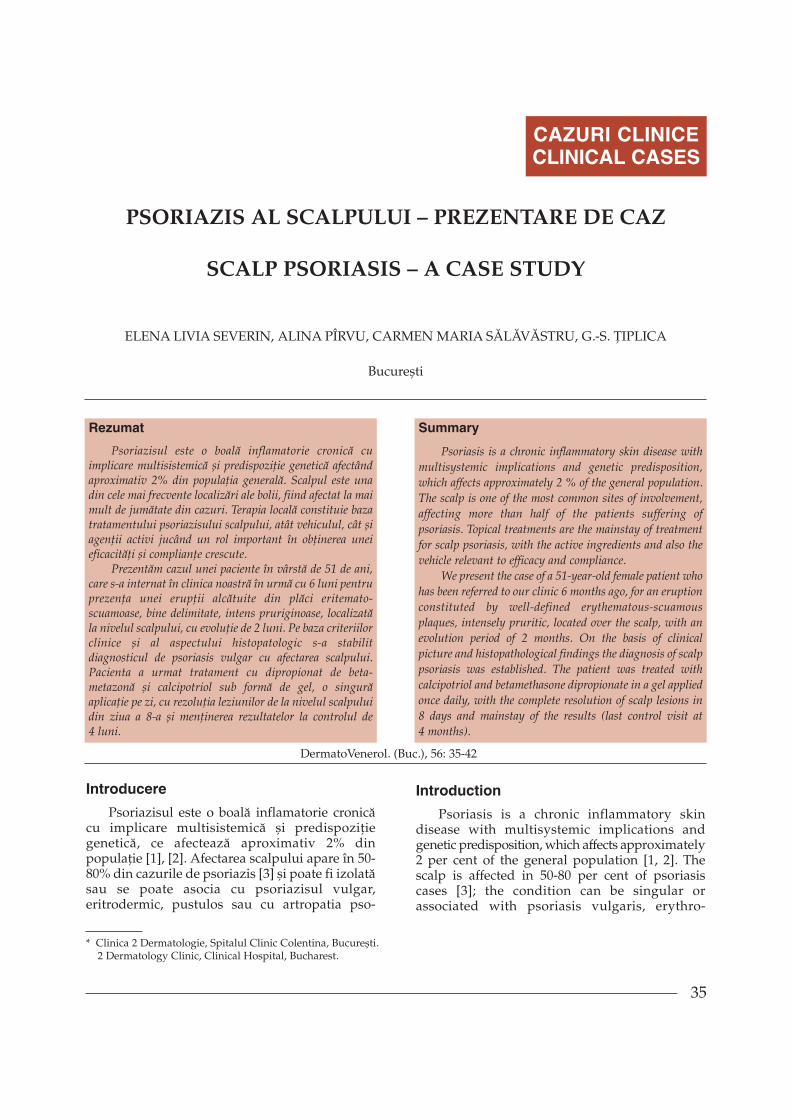
Examenul clinic general la internare a fost înlimite normale, cu excepþia leziunilor cutanate dela nivelul scalpului ºi a unei stãri depresive.Examenul dermatologic a decelat plãci eritemato-scuamoase, bine delimitate, cu contur policiclic,acoperite de scuame alb-argintii, pruriginoase,ocupând aproximativ 70% din suprafaþa scalpu-lui (figura 1). Pacienta nu prezenta în momentulconsultului alte leziuni cutanate, modificãriunghiale sau acuze articulare iar istoricul familialpentru psoriazis era negativ. Psoriasis ScalpSeverity Index (PSSI) la internare = 24. Derma-tology Life Quality Index (DLQI) în momentulprezentãrii = 11 (afectare moderatã a calitãþiivieþii).
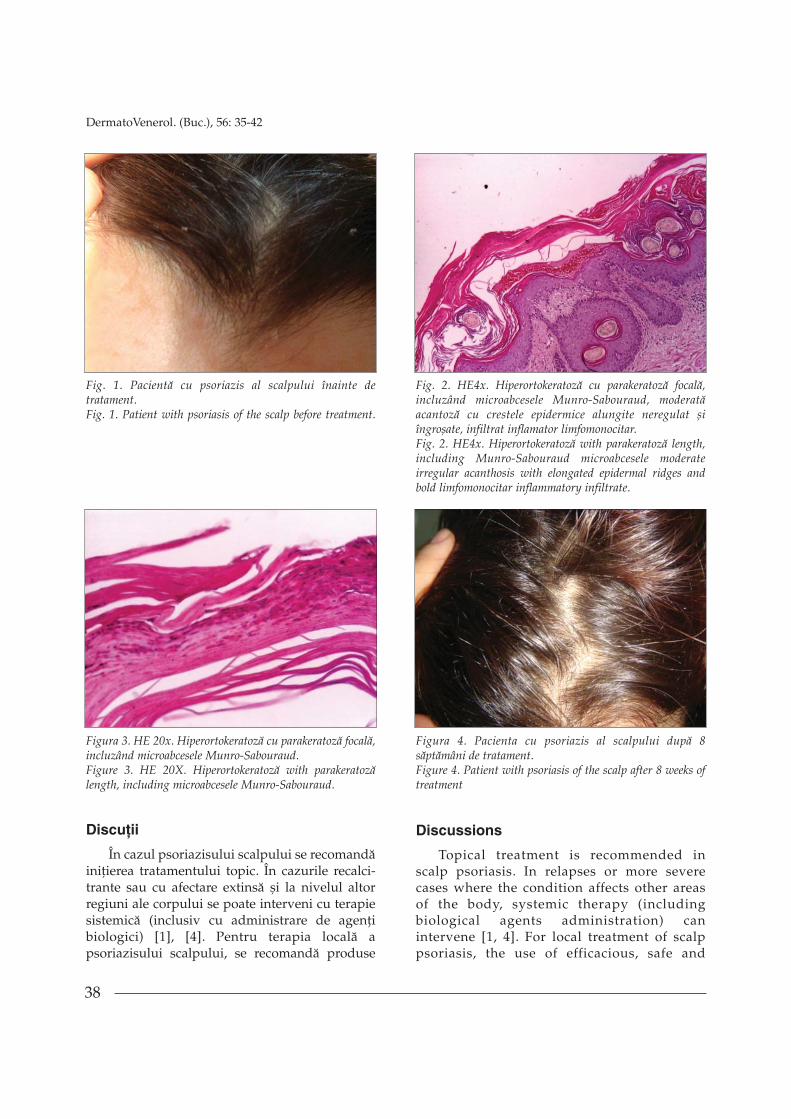
Din punct de vedere al analizelor delaborator, parametri hematologici ºi biochimiciau fost în limite normale. Examenul micologicmicroscopic direct efectuat la nivelul leziunilor afost negativ. Examenul histopatologic de lanivelul unei leziuni a scalpului a evidenþiatmarcatã hiperortokeratozã, parakeratozã focalã,incluzând numeroase colecþii de neutrofile întrestraturile de keratinã (microabcese Munro-Sabouraud), arii de hipo-agranulozã, moderatãacantozã cu creste epidermice alungite neregulatºi îngroºate, atrofie suprapapilarã focalã, moderatinfiltrat inflamator limfomonocitar cu foarte rareeozinofile, predominant perivascular în dermulsuperficial, hiperemie, cu vase capilare ectaziate,edem ºi moderatã fibrozã în dermul superficial(figurile 2 ºi 3).
Diagnosticul stabilit pe baza criteriilor cliniceºi histopatologice a fost de psoriazis vulgarsporadic, cu leziuni în plãci, afectând scalpul.
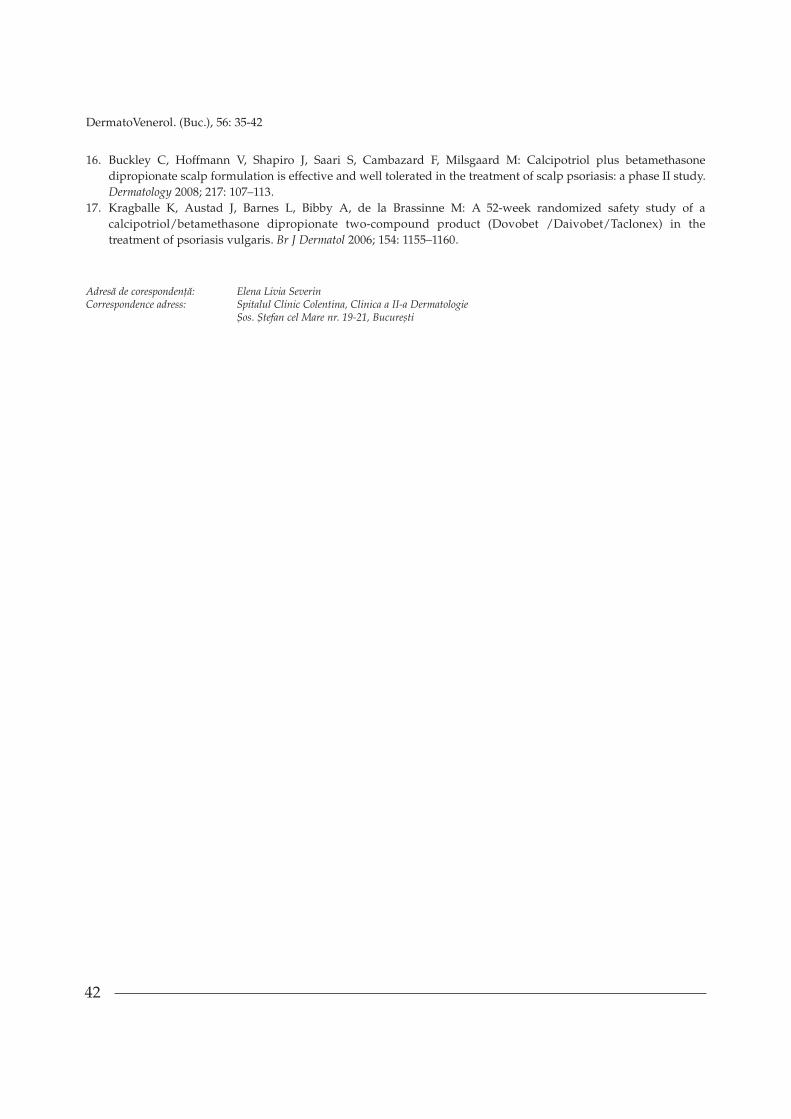
Având în vedere localizarea ºi particularitateaevoluþiei leziunilor de la acest nivel, s-a optatpentru tratament cu dipropionat de beta-metazonã ºi calcipotriol sub formã de gel (topiccombinat special conceput pentru scalp). S-arecomandat aplicarea acestui produs o datã pe zi,în strat subþire la nivelul leziunilor, cu controaleperiodice pentru evaluarea eficacitãþii trata-mentului. La 3 zile de la debutul tratamentuluipacienta a semnalat dispariþia pruritului, PSSI afost 16, iar DLQI = 8. Dispariþia leziunilor a fostraportatã de pacientã în ziua 8-a. Medicaþiatopicã a fost opritã în ziua a 10-a (data consul-tului dermatologic). La controalele ulterioare (4,6, 8 ºi respectiv 16 sãptãmâni) s-a constatatmenþinerea remisiunii leziunilor (figura 4).
General clinical examination on hospitalizationhas yielded results within normal limits, with theexception of scalp cutaneous lesions and of astate of depression. Dermatological examinationhas shown well-defined erythematous-scuamousplaques with polyciclyc margins covered bywhite-silverish pruritic scales covering about 70per cent of scalp surface (Fig. 1). The moment thepatient referred to our clinic, she did not presentother cutaneous lesions, nail modifications orarticular conditions and family history did notcomprise cases of psoriasis. Psoriasis ScalpSeverity Index (PSSI) upon hospitalization = 24.Dermatology Life Quality Index (DLQI) = 11(moderate life quality alteration).
Laboratory analyses have revealedhematologic and biochemical parameters withinnormal limits. Direct microscopic mycologicalexamination of lesions yielded negative results.Histopathological examination of a scalp lesionhas shown marked hyperorthokeratosis, focalparakeratosis, including numerous clusters ofneutrophils in-between layers of keratin (Munro-Sabouraud microabcesses), area of hypo-agranulosis, moderate acanthosis with irregularand thickened longish edges, focal suprapapillaratrophy, moderate lymphomonocyteinflammatory infiltrate with very scarceeosinophils, predominantly perivascular in thesuperficial dermis, hyperaemia with highlyectasised capillary vessels, oedema and moderatefibrosis in the superficial dermis (Fig. 2 and 3).
On the basis of clinical picture andhistopathological findings the diagnosis ofsporadic psoriasis vulgaris with plaque lesionsinvolving the scalp was established.
Taking into account the localisation andpecularities of lesions development in this area ofthe body, the treatment chosen wasbetamethasone dipropionate and calcipotrioladminsitration as gel (a topical compositionespecially created for the scalp). One applicationper day, in a thin layer on the lesion wasrecommended, plus periodical control visits inorder to evaluate treatment efficacy. Three daysafter treatment started the patient reportedpruritus resolution, PSSI = 16 and DLQI = 8.Lesions resolution was reported after the eighthday. Topical medication was stopped in day 10(dermatological consulation date). Subsequentcontrols (4, 6, 8 and 12 weeks later) haveconfirmed mainstay of the results (Fig. 4).
38
DermatoVenerol. (Buc.), 56: 35-42
Discuþii
În cazul psoriazisului scalpului se recomandãiniþierea tratamentului topic. În cazurile recalci-trante sau cu afectare extinsã ºi la nivelul altorregiuni ale corpului se poate interveni cu terapiesistemicã (inclusiv cu administrare de agenþibiologici) [1], [4]. Pentru terapia localã apsoriazisului scalpului, se recomandã produse
Discussions
Topical treatment is recommended inscalp psoriasis. In relapses or more severecases where the condition affects other areasof the body, systemic therapy (includingbiological agents administration) canintervene [1, 4]. For local treatment of scalppsoriasis, the use of efficacious, safe and
Fig. 1. Pacientã cu psoriazis al scalpului înainte detratament.Fig. 1. Patient with psoriasis of the scalp before treatment.
Fig. 2. HE4x. Hiperortokeratozã cu parakeratozã focalã,incluzând microabcesele Munro-Sabouraud, moderatãacantozã cu crestele epidermice alungite neregulat ºiîngroºate, infiltrat inflamator limfomonocitar.Fig. 2. HE4x. Hiperortokeratozã with parakeratozã length,including Munro-Sabouraud microabcesele moderateirregular acanthosis with elongated epidermal ridges andbold limfomonocitar inflammatory infiltrate.
Figura 3. HE 20x. Hiperortokeratozã cu parakeratozã focalã,incluzând microabcesele Munro-Sabouraud.Figure 3. HE 20X. Hiperortokeratozã with parakeratozãlength, including microabcesele Munro-Sabouraud.
Figura 4. Pacienta cu psoriazis al scalpului dupã 8sãptãmâni de tratament.Figure 4. Patient with psoriasis of the scalp after 8 weeks oftreatment

39
DermatoVenerol. (Buc.), 56: 35-42
eficiente, sigure ºi acceptabile din punct devedere cosmetic pentru aceastã localizare [8], [9].
Studiile meta-analitice pentru agenþii topiciutilizaþi în tratamentul psoriazisului în plãci aidentificat în total 42 de studii placebo-controlate,din care doar 7 s-au concentrat pe psoriazisulscalpului [3], [10].
Arsenalul terapeutic pentru psoriazisulscalpului este variat (keratolitice, reductoare,fototerapie - inclusiv laser excimer), cei maifrecventi agenþi utilizaþi fiind corticosteroizii ºiderivaþii de vitamina D, a cãror eficienþã a fostdoveditã atât în monoterapie, cât ºi în combinaþii,în numeroase studii clinice [11], [12], [13].
Calcipotriolul, derivat de vitamina D, îºiexercitã efectele benefice în psoriazis prininhibarea proliferãrii epidermice ºi a inflamaþiei,precum ºi prin stimularea keratinizãrii normale[8], [14]. Acest agent terapeutic este utilizat înpsoriazisul scalpului din anul 1992 iar eficacitateape termen lung ºi siguranþa au fost bine stabilite[11].
Corticosteroizii fac parte din principaliiagenþi topici utilizaþi în psoriazisul scalpului depeste 30 de ani. Efectele corticosteroizilor topiciinclud efectele antiinflamatorii ºi imuno-modulatorii precum ºi scãderea activitãþiimitotice epidermice [15]. Efectele adverse alecorticosteroizilor topici sunt bine cunoscute ºi potfi împãrþite în locale (ex. telangiectazii, atrofieacnee, vergeturi) ºi sistemice (supresia axuluihipotalamo- hipofizar). [8]. Corticosteroizii suntadesea combinaþi cu alþi agenþi (inclusiv derivaþiide vitamina D), în încercarea de a beneficia deefectele lor complementare [8]. Încã din 2001,combinaþia calcipotriolului cu corticosteroidulpotent dipropionat de betametazonã a devenit untratament recunoscut în psoriazisul vulgar culocalizare la nivelul trunchiului ºi extremitãþilor.Dipropionatul de betametazonã realizeazã oameliorare rapidã a simptomelor ºi previneiritaþia localã provocatã de calcipotriol, iaradãugarea acestuia din urmã contribuie laeficientizarea terapiei ºi permite reducereacantitãþii de corticosteroid necesarã obþineriirãspunsului favorabil [11].
Recent a fost conceputã o combinaþie a celordoi agenþi într-un vehicul – gel – adaptat terapieipsoriazisului de la nivelul scalpului (denumirecomercialã: Xamiol). Studiile iniþiale aratã cã
cosmetically accepted products comes highlyrecommmended [8, 9].
Meta-analytical studies conducted on topicalagents used in plaque psoriasis treatment haverevealed a total of 42 placebo-controlled studies,out of which only 7 were focussed on scalppsoriasis [3, 10].
Therapeutical methods used in scalp psoriasvary from keratolytics to reducing agents andphototherapy (excimer laser included). Theagents most frequently used are corticosteroidsand vitamin D derivatives, whose efficacy hasbeen proved, both in monotherapy and incombinations, by numerous clinical studies [11,12, 13].
Calcipotriol, a vitamin D derivative, exertsbeneficial effects on psoriasis by inhibitingepidermic and inflammation proliferation and bystimulating normal keratinisation [8, 14]. It hasbeen used in scalp psoriasis treatment beginningwith 1992 and its long-term efficacy and safetyhas long been established [11].
Corticosteroids also belong to the main groupof topical agents used for over 30 years in scalppsoriasis treatment. Among others, they haveanti-inflammatory and immunomodulatingeffects and decrease epidermic mitotic activity[15]. Adverse reactions to topical corticosteroidsare well known and can be divided into local (e.g.telangiectases, acne atrophy, striae) and systemicones (suppression of the hypothalamo-hypophyseal axis) [8]. Corticosteroids are oftenadministered in combination with other agents(including vitamin D derivatives), in the attemptto benefit from their complementary effects [8].As far as 2001, the combination betweencalcipotriol and betamethasone dipropionate, apotent corticosteroid, has become a treatmentrecommended in psoriasis vulgaris of the trunkand limbs. Betamethasone dipropionate achievesrapid amelioration of symptoms and preventslocal irritation caused by calcipotriol, while anaddition of the latter contributes to a moreefficient therapy by reducing the quantity ofcorticosteroid necessary to obtain a favourableresult [11].
More recently this combination wasformulated as gel – trade name Xamiol – ,adapted for scalp psoriasis treatment. Initialstudies show that this new formula is efficacious,

40
DermatoVenerol. (Buc.), 56: 35-42
aceastã nouã formulã este eficientã, bine toleratãºi superioarã monoterapiei cu dipropionat debetametazonã sau calcipotriol, dupã 8 sãptãmânide tratament [16]. Având în vedere faptul cãpsoriazisul scalpului este o afecþiune cronicã, cuperioade de exacerbare ºi remisiune, suntnecesare cure repetate de tratament. Pentruinvestigarea siguranþei administrãrii pe termenlung a acestui tratament în psoriazisul scalpului,Luger et al. (2008) au realizat un studiu în care ºi-au propus testarea siguranþei administrãriicombinaþiei dipropionat de betametazonã ºicalcipotriol pe o perioadã de 52 de sãptãmâni.Printre rezultatele studiului se regãseºte ºi lipsaatrofiei cutanate în grupul care a utilizatcombinaþia de agenþi topici. Incidenþa scãzutã areacþiilor adverse de tip corticosteroidic (ex.,telangiectazii, acnee, rozacee) ar avea mai multeexplicaþii: comparativ cu produsele de tipcorticosteroid, cantitatea de produs combinataplicatã ºi consecutiv, gradul de expunere lacorticosteroid, este mai redusã; produsele cucorticosteroizi disponibile fie se aplicã de douãori pe zi, fie au o potenþã superioarãdipropionatului de betametazonã [8]. Un studiuanterior, având ca scop testarea utilizãrii petermen lung a produsului combinat dipropionatde betametazona ºi calcipotriol sub formã deunguent a demonstrat, de asemenea, o incidenþãfoarte scãzutã a reacþiilor adverse de tipcorticosteroid [17]. Incidenþa pruritului, unul dincele mai supãrãtoare simptome ale psoriazisuluiscalpului, a fost mult scãzutã în grupuldipropionat de betametazonã ºi calcipotriol (3,6%), comparativ cu grupul calcipotriol (10%) [8]. ªila controalele de dupã 6 luni, respectiv 12 luni detratament s-a constatat lipsa acumulãrii tisulare aprodusului, care ar fi putut duce la schimbareaprofilului sãu de siguranþã dupã expunerirepetate. Pânã în prezent, în tratamentulpsoriazisului scalpului, utilizarea produsuluicombinat dipropionat de betametazonã ºicalcipotriol s-a dovedit mai eficientã comparativcu monoterapia cu alþi agenþi (calcipotriol o datãsau de douã ori pe zi, alþi corticosteroizi topici),bine toleratã pe o perioadã lungã de timp (pânã la52 de sãptãmâni) ºi cu o incidenþã scãzutã areacþiilor adverse atât generale, cât ºi de tipcorticosteroidic [8], [15], [17].
well tolerated and has proved superior after 8weeks of administration to monotherapyconsisting of betamethasone dipropionate orcalcipotriol [16]. Since scalp psoriasis is a chronicdisease, with aggravation and remission periods,repeated cures are recommended. In 2008, Lugeret al. conducted an investigation on the safety oflong-term administration of this product in scalppsoriasis over a period of 52 weeks. The studyreveales, among others, the absence of cutaneousatrophy in the group that used the combination.Low incidence rate of adverse corticosteroidicreactions (e.g. telangiectases, acne, rush) can beascribed to a multitude of causes: as compared tocortocosteroid-type products, the quantity ofcosticosteroid applied and, by consequence, thedegree of exposure to it is lower; costicosteroid-based products available on the market are eitherapplied twice a day or are more potent thanbetamethasone propionate [8]. A studyperformed beforehand with the purpose oftesting betamethasone propionate andcalcipotriol combination formulated as ointmenthas also shown a very low incidence of adversecorticosteroidic reactions [17]. Pruritus, one of themost disturbing symptoms in scalp psoriasis,occurred much more seldom in the group ofpatients who were administered the combinationof betamethasone propionate and calcipotriol (3.6per cent) as compared to calcipotriol group (10per cent) [8]. Control visits after 6 and 12 monthsof treatment also confirmed absence of productaccumulation in the tissues, which could have ledto a change in the safety profile after repeatedexposure. Up to the present, betamethasonepropionate and calcipotriol combination hasproved more efficacious as compared tomonotherapy with other agents (calcipotrioladministered once or twice a day, other topicalcorticosteroids). It is also better tolerated in long-term therapy (up to 52 weeks) and triggers lessadverse reactions, both general and ofcorticosteroidic type [8, 15, 17].
Conclusions
Local therapy is the basic treatment in scalppsoriasis but, as a rule, preparations are hard toapply due to the hair and the thick squamas thatblock the penetration of active therapeuticalsubstances. Recently, a lipophilic gel containing

41
DermatoVenerol. (Buc.), 56: 35-42
Concluzii
Terapia localã constituie baza tratamentuluiîn psoriazisul scalpului, însã, de regulã, pre-paratele sunt dificil de aplicat datoritã pãrului ºiscuamelor groase care reprezintã un obstacol înpãtrunderea substanþelor terapeutice active.Recent a fost introdusã pe piaþã combinaþiadipropionat de betametazonã 0,05% ºi calci-potriol 0,005% cu formulã special conceputãpentru utilizare la nivelul scalpului – gel lipofilic.Pânã în prezent utilizarea acestui produscombinat s-a dovedit eficientã ºi cu o incidenþãscãzutã a reacþiilor adverse.
Intrat în redacþie: 18.02.2011
0.05 per cent betamethasone dipropionate and0.005 per cent calcipotriol has been especiallyconceived for scalp treatment. Until now, thiscombination has proved efficacious, and theincidence rate of adverse reaction has beeen low.
Received: 18.02.2011
Bibliografie/Bibliography
1. Guenther LC. Treatments for Scalp Psoriasis with Emphasis on Calcipotriol Plus Betamethasone Dipropionate Gel(Xamiol®), Skin Therapy Letter 14 (4) (aprilie 2009), www.SkinCareGuide.com la 10 februarie 2011.
2. Christophers E. Psoriasis: epidemiology and clinical spectrum. Clin Exp Dermatol 26 (4): 314-20 (2001 Jun).3. Papp K, Berth-Jones J, Kragballe K, et al. Scalp psoriasis: a review of current topical treatment options. J Eur Acad
Dermatol Venerol 21 (9): 1151-60 (2007 Oct).4. Wozel G. Psoriasis treatment in difficult locations: scalp, nails and intertriginous areas. Clin Dermatol 26 (5): 448-
59 (2008 Sep-Oct).5. Schoorl WJ, van Baar HJ, van de Kerkhof PC. The hair root pattern in psoriasis of the scalp. Acta Derm Venereol
72(2):141-2 (1992).6. Handa S. Newer trends in the management of psoriasis at difficult to treat locations: Scalp, palmoplantar disease
and nails. Indian J Dermatol Venereol Leprol 2010; 76: 634-44.7. Jemec GBE, Ganslandt C, Ortonne JP, Poulin Y, Burden AD: A new scalp formulation of calcipotriene plus
betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: arandomized double-blind, controlled trial. J Am Acad Dermatol 2008; 59: 455–463.
8. Luger, T.A., Cambazard, F, Larsen, G., Bourcier, M., Gupta, G., Clonier, F., Kidson, P., Shear, N.H. A Study of theSafety and Efficacy of Calcipotriol and Betamethasone Dipropionate Scalp Formulation in the Long-TermManagement of Scalp Psoriasis. Dermatology 2008; 217: 321–328.
9. Feldman SR, Housman TS: Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J ClinDermatol 2003; 4: 221–224.
10. Mason J, Mason AR, Cork MJ. Topical preparations for the treatment of psoriasis: a systematic review. Br JDermatol 2002; 146: 351–364.
11. Carine J.M. van der Vleuten, Peter C.M. van de Kerkhof. Management of Scalp Psoriasis Guidelines forCorticosteroid Use in Combination Treatment. Drugs 2001; 61 (11): 1593-1598.
12. Lebwohl M, Ting PT, Koo JY: Psoriasis treatment: traditional therapy. Ann Rheum Dis 2005; 64:ii83–ii86.13. Warwick L. Morison, Darleen F. Atkinson, Lucille Werthman. Effective treatment of scalp psoriasis using the
excimer (308 nm) laser. Photodermatol Photoimmunol Photomed 2006; 22: 181–183.14. Kragballe K, Wildfang IL: Calcipotriol (MC 903), a novel vitamin D3 analogue stimulates terminal differentiation
and inhibits proliferation of cultured human keratinocytes. Arch Dermatol Res 1990; 282: 164–167.15. Kragballe, K., Hoffmann, V., Ortonne, J.P. Efficacy and safety of calcipotriol plus betamethasone dipropionate
scalp formulation compared with calcipotriol scalp solution in the treatment of scalp psoriasis: a randomizedcontrolled trial. British Journal of Dermatology 2009 161, pp159–166.
42
DermatoVenerol. (Buc.), 56: 35-42
16. Buckley C, Hoffmann V, Shapiro J, Saari S, Cambazard F, Milsgaard M: Calcipotriol plus betamethasonedipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study.Dermatology 2008; 217: 107–113.
17. Kragballe K, Austad J, Barnes L, Bibby A, de la Brassinne M: A 52-week randomized safety study of acalcipotriol/betamethasone dipropionate two-compound product (Dovobet /Daivobet/Taclonex) in thetreatment of psoriasis vulgaris. Br J Dermatol 2006; 154: 1155–1160.
Adresã de corespondenþã: Elena Livia SeverinCorrespondence adress: Spitalul Clinic Colentina, Clinica a II-a Dermatologie
ªos. ªtefan cel Mare nr. 19-21, Bucureºti