ultrasonographic diagnosis of acute...
TRANSCRIPT
Original papers
Ultrasonographic diagnosis of acute appendicitis
Călin Moş1, Teodor Ile2, Monica Hălbac2, Laura Chiş2, Sorin Vesa2, Ştefan Andor2
1University of Oradea, Faculty of Medicine and Pharmacy, Romania2County Hospital, Beiuş, Romania
Address for correspondence: Dr. Călin Moş Str. Andrei Şaguna nr.1 415200, Beiuş, jud. Bihor, România e-mail: [email protected]
AbstractIntroduction. Appendectomy, the most frequent surgical intervention, has 20-30% rate of negative appendectomy mostly
because of 30-45% cases with unspecifi c clinical examination. The objective of this study was to determine the contribution of ultrasonography in acute appendicitis (AA) diagnosis in patients with abdominal pain in the right lower quadrant.
Material and method. A number of 262 patients with clinical suspicion of AA were investigated. The positive diagnosis criteria were considered to be the appendix external diameter >6 mm, appendix wall thickness >3 mm, partial or total absence of wall stratifi cation, coprolites or/and liquid in excess in the appendix lumen, hypervascularization of appendix wall, echogenic-ity enhanced and hyperemia in periappendicular mesenteric fat, periappendicular collection (abscess) or peritoneal collection (peritonitis).
Results. Appendix was identifi ed by ultrasonography in 199 out of 262 of patients (75.9%). Normal appendix was less visual-ized (in 61.9%) comparing to pathologic appendix (91.3%). Ultrasonography demonstrated an 89.4% sensibility, 95.2% specifi -city, positive predictable value 95.5% and negative predictable value 88.9% in the detection of AA. Preoperative ultrasonographic examination in patients with abdominal pain of the right lower quadrant leads to 9.9% negative rate of appendectomies.
Conclusions. In cases of abdominal pain located in the right lower quadrant, ultrasonography is a quick non-invasive and low cost method which can contribute to an early positive diagnosis and also a decrease in the number of unnecessary appendectomies.
Key-words: acute appendicitis, ultrasound, diagnosis
RezumatIntroducere. Apendicectomia, cea mai frecventă intervenţie chirurgicală, are o rată de 20-30% de apendicectomii negative,
in primul rind deoarece in aproximativ 30-45% cazuri examenul clinic este nespecifi c. Scopul studiului este de a determina contribuţia ecografi ei în diagnosticul apendicitei acute la cazurile cu sindrom dureros de fosă iliacă dreaptă.
Material şi metodă. S-au evaluat ecografi c 262 de pacienţi cu suspiciunea clinică de apendicită acută. Criteriile ecografi ce de diagnostic pozitiv au fost: diametrul extern al apendicelui peste 6 mm, grosimea a peretelui peste 3 mm, dispariţia parcelară sau totală a stratifi cării pereţilor, prezenţa în lumen a coproliţilor şi/sau a lichidului în exces, hipervascularizaţia peretelui apen-dicular, creşterea ecogenităţii şi hiperemia grăsimii mezenterice periapendiculare, prezenţa unei colecţii periapendiculare (abces) sau peritoneale (peritonită).
Rezultate. Apendicele a fost identifi cat ecografi c la 199 dintre cei 262 de pacienţi (75,9%). Apendicele normal a fost mai rar vizualizat (61,9%) comparativ cu cel patologic (91,3%). Ecografi a are sensibilitate de 89,4%, specifi citate de 95,2%, acurateţe de 94,3%, valoare predictivă pozitivă de 95,5% şi valoare predictivă negativă de 88,9% în detectarea apendicitei acute. Examinarea ecografi că preoperatorie a pacienţilor cu suspiciunea clinică de apendicită acută a dus la o rata de apendicectomii negative de doar 9,9%.
Concluzii. În cazul unei simptomatologii dureroase de fosă iliacă dreaptă, ecografi a este o metodă neinvazivă, rapidă şi cu preţ de cost scăzut care poate să contribuie la un diagnostic pozitiv precoce, la diminuarea ratei de apendicectomii cu apendice normal şi la clarifi carea diagnosticului diferenţial.
Cuvinte cheie: apendicită acută, ecografi e, diagnostic
Acute appendicitis (AA) is the most common acute surgical condition [1], about 7% of the population having an appendectomy during their lifetime [2]. Maximum in-cidence is between 6 and 30 years [3,4]. In about 30-45% of cases the clinical evaluation is unspecifi c [5].
Medical Ultrasonography2009, Vol. 11, no. 3, 7–18

2 Călin Moş et al Ultrasonographic diagnosis of acute appendicitis
The appendix is a worm-shaped pouch originating from the lowest part of cecum. It usually has an intraperi-toneal position (anterior or retrocecal) in contact with the anterior parietal peritoneum. A wide mesentary permits the appendix rotation in several positions. So in 30% of cases the appendix is placed in the pelvis, retrocecal or retroperitoneal. These positions can modify clinical signs and symptoms of AA [6].
AA are caused by obstruction of the appendix lumen through several causes: lymph hyperplasia (especially in children and young adults in viral infections, mononucle-osis, gastroenteritis or ileocolitis), coprolites, parasites, foreign body, Crohn’s disease or neoplasm [5,7,8,9].
If the diagnosis of AA is based only on clinical and laboratory fi ndings, about 20-30% of appendectomies are not confi rmed at pathologic examination [9,10,11]. In AA an early diagnosis is crucial to reduce the risk of complications (perforation, occlusion, sepsis) which can increase the mortality especially at extreme ages [1].
In a small number of patients with AA (between 1-10%) the appendix infl ammation is discrete, clinical signs are blurred and rapidly subsided, and the clinical evolution is rapidly to spontaneous remission. These are called abortive appendicitis, limited appendicitis or spontane-ous healing appendicitis [12,13]. In atypical cases of AA, the surgeon have to choose between instant and delayed surgery. The ultrasonography (US) of abdomen and ap-pendix region can help the surgeon to take the proper decision.
The advantages of US in AA diagnosis are the low cost, the lack of irradiation, and the possibility to exam-ine carefully and repetitively the maximum sensibility zone. The main disadvantage of the US is the operator-dependence and the diffi culty in scanning obese patients. [14,15,16]. An experienced operator, with the aid of a modern devices (with high resolution probe), could have a sensitivity, accuracy and specifi city around 90% in US diagnostic of AA. Also, in the patients with appendicitis-like symptoms, US can reveal the correct diagnosis in almost 70-80% of cases [17].
The aim of our study was to evaluate the contribution of the US for the positive and differential diagnosis of the AA, in patients with abdominal pain localized in the right lower quadrant.
Material and method
The study comprised 262 patients (136 males, 126 females, aged between 4–73) presenting with right lower quadrant abdominal pain at the Beius County Hospital between December 2007 and July 2009. They all had clinical suspicion of AA. US was performed by a doc-
tor (CM) with experience in gastrointestinal tract US. A Voluson 730 PRO General Electric Kretz Technik ul-trasound machine with multifrequence probe (1.5-18.5 MHz) was used.
The examination protocol, based on graded compres-sion describe by Puylaert [18] included:
1. Convex probe use. The US examination started with an abdominal general scanning (to exclude an ex-traappendicular pathology) using a 1.5-4.5 MHz or 4.0-8.5 MHz convex probe, depending on body weight. For obese patients the same convex probe was used for ap-pendix region examination.
2. Linear probe use. For the examination of the ap-pendix region we used a 5-18.5 MHz linear probe. Ac-cording to the Puylaert technique [18,19] a graded com-pression was exerted with the transducer, to dislocate the air and to identify the most painful region. The landmarks of the region (cecum, last portion of the ileum, iliopsoas muscle, iliac vessels and appendix) were identifi ed. The examination began with sections from the ascending co-lon to the cecum. After the identifi cation of the cecum base, longitudinal sections from the lateral to the median part of the cecum were made. Usually the appendix was identifi ed in the maximum painful zone. If the appendix was not identifi ed in its normal position, the examination continued to explore the retrocecal, retrocolic, pelvic and retroileal regions using the appendix base as a landmark (always the base was situated in the same position).
We used US in gray scale for morphological analysis and Doppler US for the examination of appendix vas-cularization (with a small velocity scale and 70-120 Hz parietal fi lter).
US exclusion criteria for AA were an US unidentifi -able appendix or a compressible appendix, oval shape in transverse section, with external diameter under 6 mm, wall thickness under 3 mm, wall layers and normal peri-appendicular mesenteric fat. US positive diagnosis cri-teria for AA were considered the external diameter of the appendix over 6 mm, the appendix wall thickness over 3 mm, total or partial wall layers nonvisualisation, copro-lites and/or fl uid excess into appendix lumen, hypervas-cularization of the appendix wall, enhance of echogenic-ity and hyperemia of the periappendicular mesenteric fat, periappendicular collection (abscess) or peritoneal col-lection (peritonitis).
The histopathological examination of the appendix was performed in all surgical cases.
The result was considered true positive when the US diagnosis concurred with the histopathological fi ndings and true negative when the histopathology for AA was negative or there was no relapse in 2 weeks of follow up of the nonsurgical patients.
3Medical Ultrasonography 2009; 11(3): 7–18
The result was considered false positive when there was a US diagnosis of AA with normal histopathologi-cal fi ndings in the appendix, and false negative when US found a normal or unidentifi able appendix with positive histopathology for AA.
A 2x2 table and χ2 test were used for the evaluation of the results. The sensitivity, specifi city, accuracy, positive and negative predictive values were determinate (PPV, NPV). The confi dence interval was 95%.
Results
In the majority of the cases the appendix was identi-
fi ed in about 1-3 minutes. An unidentifi ed US appendix was considered a normal appendix. From 262 examined patients, 141 were submitted to appendicectomy. In 127 patients there was a histological confi rmation of AA. In 14 patients the histological examination was negative resulting 9.9% appendicectomies for a normal appendix (tab I, tab II).
The clinical situations which led to false positive and false negative results are presented in table III.
The statistical data analysis shows 89% sensibil-ity, 95.2% specifi city, 94.3% accuracy, 95.5% PPV and 88.9% NPV of the US in diagnosis of AA.
Table I. US identifi cation of the appendix and the therapy of the patients with pain in the right lower quadrant (RLQ); AA – acute appendicitis
US fi ndings Number of patients with pain RLQ (total 262)
Patients with appendectomy (total 141)
Patients with conservative therapy (total 120)
US diagnosis of AA(total 118)
Identifi ed appendix
199(75,9%)
120(89,4%)
79(65,8%)
103(87,3%)
Unidentifi ed appendix
63(24.1%)
21(10,6%)
41(34,2%)
15(12,7%)
Table II. US diagnosis and the therapy of the patients with pain in the right lower quadrant (RLQ); AA- acute appendicitis
US diagnosis Number of patients with pain in RLQ (total 262)
Patients with appendectomy(total 141)
Patients with conservative therapy (total 120)
US diagnosis of AA(total 118)
AA 127(48,5%)
127(90,1%)
0(0%)
112(94,9%)
Without AA 135(51,5%)
14(9,9%)
120(100%)
6(5,1%)
Table III. The causes of false positive or false negative results at US
Outcome type The cause of false outcome Number of cases
False positive
• hydrosalpings• mucocele with pseudomyxoma peritonei in small quantity• terminal ileum segmental necrosis• Meckel’s diverticulitis• cecal diverticulitis• ovarian torsion
Total
1111116
False negative
Appendix lack of identifi cation without real associated pathology• obesity• appendix point position• diffi culties in practicing graded compression• pain absence at compression in right lower quadrant
5231
Appendix lack of identifi cation with associated pathology• cecum neoplasm• infectious ileitis• hyperplastic cholecystosis with subhepatic abscess produced by appendix perforation• perforated appendix for an appendix and cecum located in left lower quadrant
1111
Total 15
4 Călin Moş et al Ultrasonographic diagnosis of acute appendicitis
Discussions
The detection by US of the normal appendix vary in published papers between 0% and 95% [18,20,21,22,23, 24,25,26], depending mostly on the US machines’ per-formances. For example, Puylaert in 1986 (in a study de-scribing the graded compression technique for appendix examination) mentions the lack of normal appendix visu-alization [18]. In a recent paper in 2005 [26] the detection rate of the normal appendix increased to 82%.
The main examination technique is one of the graded compression [18]. Some authors consider that anterior graded compression combined with posterior compres-sion can increase signifi cantly the rate of appendix detec-tion [24]. The appendix examination must be performed in its entire length because there are situations with focal infl ammation, especially on the tip of appendix. The in-complete examination of the appendix can generate false results [27].
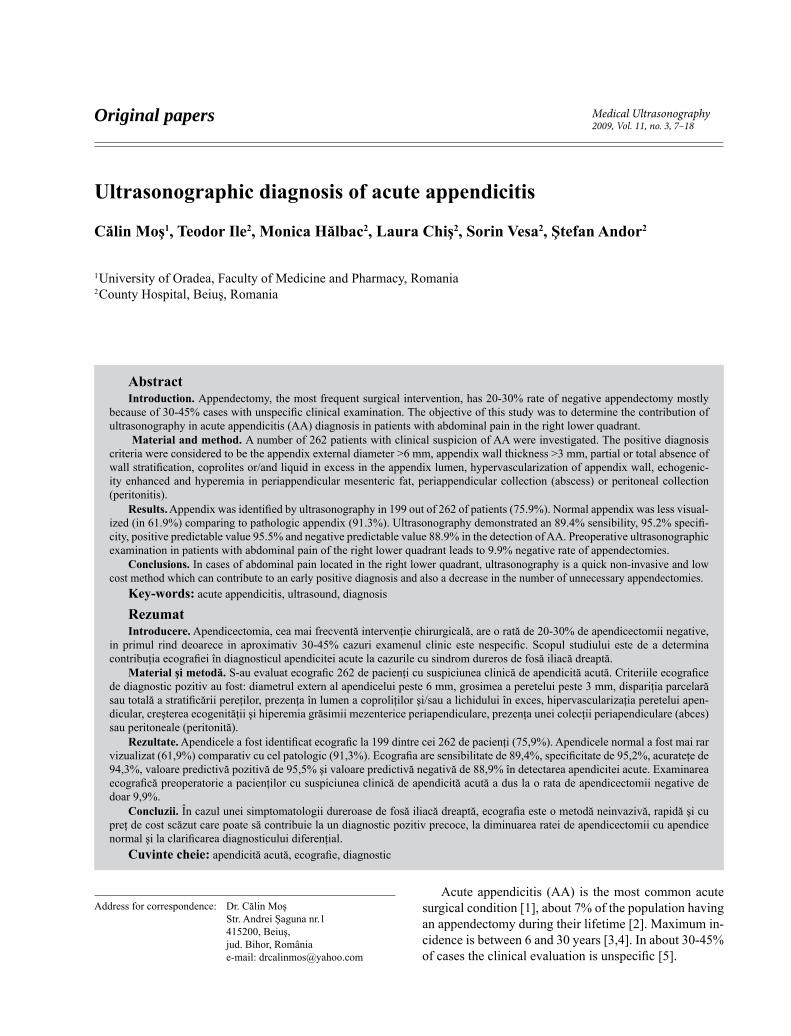
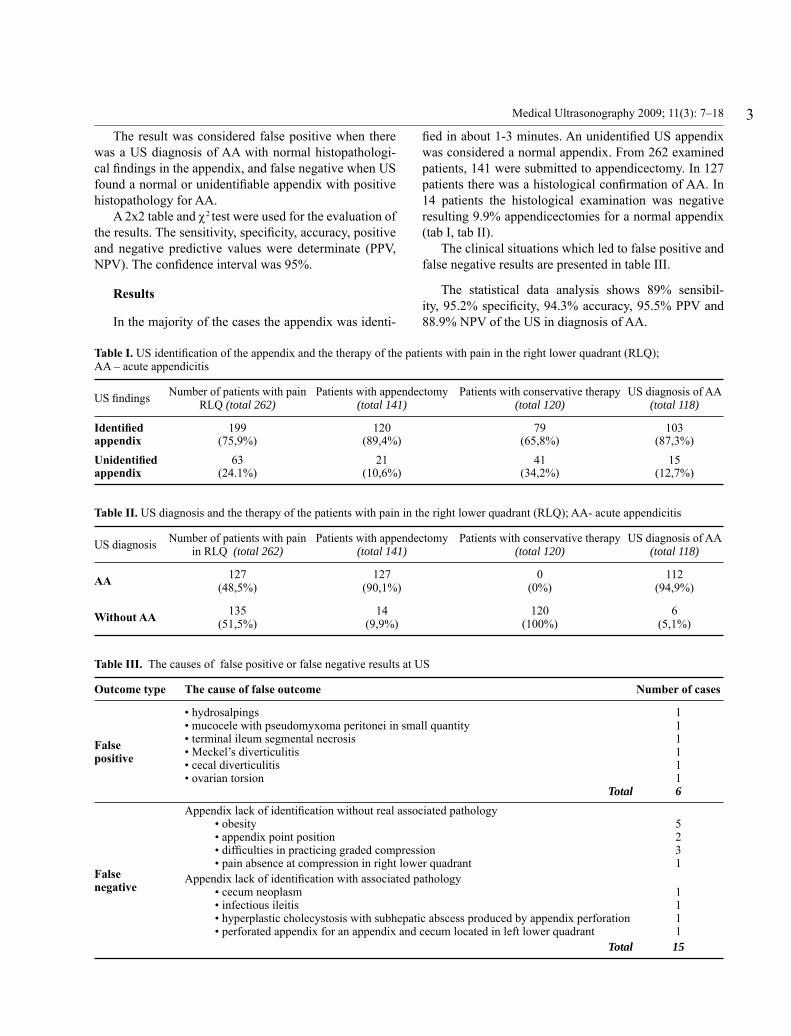
On longitudinal scan, the normal appendix is a com-pressible tubular blind-ending structure, without peristal-tic movements, no mucosal stripes and usually without visible hypervascularization. External maximum diam-eter is considered to be 4.7±1.2 mm [28] but in excep-tional cases can increase up to 8-11 mm [28]. Most of the authors considered a diameter of 6 mm as the superior value for a normal appendix (fi g 1, fi g 2) [29,30].
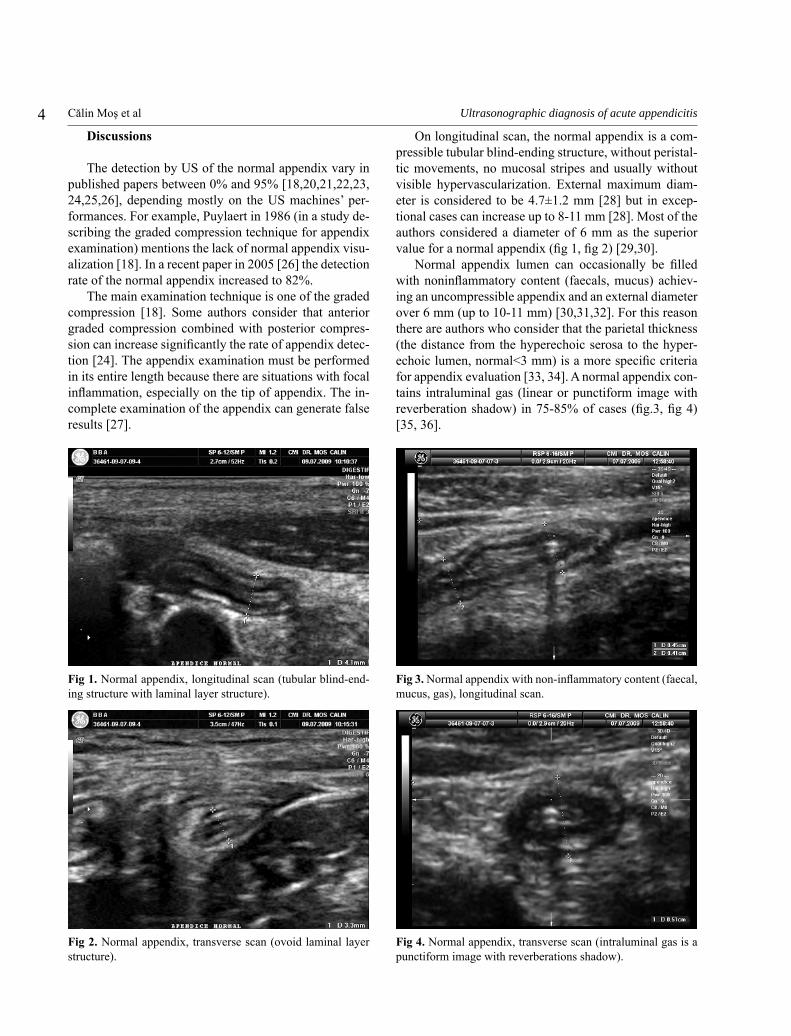
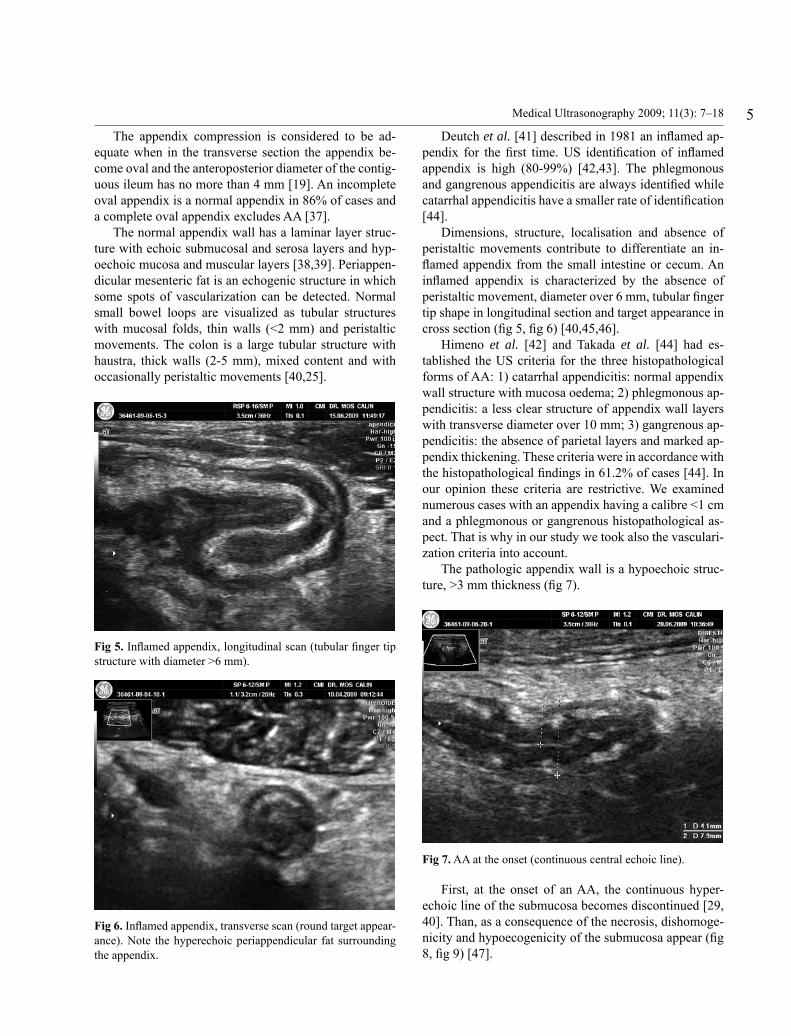
Normal appendix lumen can occasionally be fi lled with noninfl ammatory content (faecals, mucus) achiev-ing an uncompressible appendix and an external diameter over 6 mm (up to 10-11 mm) [30,31,32]. For this reason there are authors who consider that the parietal thickness (the distance from the hyperechoic serosa to the hyper-echoic lumen, normal<3 mm) is a more specifi c criteria for appendix evaluation [33, 34]. A normal appendix con-tains intraluminal gas (linear or punctiform image with reverberation shadow) in 75-85% of cases (fi g.3, fi g 4) [35, 36].
Fig 1. Normal appendix, longitudinal scan (tubular blind-end-ing structure with laminal layer structure).
Fig 2. Normal appendix, transverse scan (ovoid laminal layer structure).
Fig 3. Normal appendix with non-infl ammatory content (faecal, mucus, gas), longitudinal scan.
Fig 4. Normal appendix, transverse scan (intraluminal gas is a punctiform image with reverberations shadow).
5Medical Ultrasonography 2009; 11(3): 7–18
The appendix compression is considered to be ad-equate when in the transverse section the appendix be-come oval and the anteroposterior diameter of the contig-uous ileum has no more than 4 mm [19]. An incomplete oval appendix is a normal appendix in 86% of cases and a complete oval appendix excludes AA [37].
The normal appendix wall has a laminar layer struc-ture with echoic submucosal and serosa layers and hyp-oechoic mucosa and muscular layers [38,39]. Periappen-dicular mesenteric fat is an echogenic structure in which some spots of vascularization can be detected. Normal small bowel loops are visualized as tubular structures with mucosal folds, thin walls (<2 mm) and peristaltic movements. The colon is a large tubular structure with haustra, thick walls (2-5 mm), mixed content and with occasionally peristaltic movements [40,25].
Deutch et al. [41] described in 1981 an infl amed ap-pendix for the fi rst time. US identifi cation of infl amed appendix is high (80-99%) [42,43]. The phlegmonous and gangrenous appendicitis are always identifi ed while catarrhal appendicitis have a smaller rate of identifi cation [44].
Dimensions, structure, localisation and absence of peristaltic movements contribute to differentiate an in-fl amed appendix from the small intestine or cecum. An infl amed appendix is characterized by the absence of peristaltic movement, diameter over 6 mm, tubular fi nger tip shape in longitudinal section and target appearance in cross section (fi g 5, fi g 6) [40,45,46].
Himeno et al. [42] and Takada et al. [44] had es-tablished the US criteria for the three histopathological forms of AA: 1) catarrhal appendicitis: normal appendix wall structure with mucosa oedema; 2) phlegmonous ap-pendicitis: a less clear structure of appendix wall layers with transverse diameter over 10 mm; 3) gangrenous ap-pendicitis: the absence of parietal layers and marked ap-pendix thickening. These criteria were in accordance with the histopathological fi ndings in 61.2% of cases [44]. In our opinion these criteria are restrictive. We examined numerous cases with an appendix having a calibre <1 cm and a phlegmonous or gangrenous histopathological as-pect. That is why in our study we took also the vasculari-zation criteria into account.
The pathologic appendix wall is a hypoechoic struc-ture, >3 mm thickness (fi g 7).
First, at the onset of an AA, the continuous hyper-echoic line of the submucosa becomes discontinued [29, 40]. Than, as a consequence of the necrosis, dishomoge-nicity and hypoecogenicity of the submucosa appear (fi g 8, fi g 9) [47].
Fig 5. Infl amed appendix, longitudinal scan (tubular fi nger tip structure with diameter >6 mm).
Fig 6. Infl amed appendix, transverse scan (round target appear-ance). Note the hyperechoic periappendicular fat surrounding the appendix.
Fig 7. AA at the onset (continuous central echoic line).
6 Călin Moş et al Ultrasonographic diagnosis of acute appendicitis
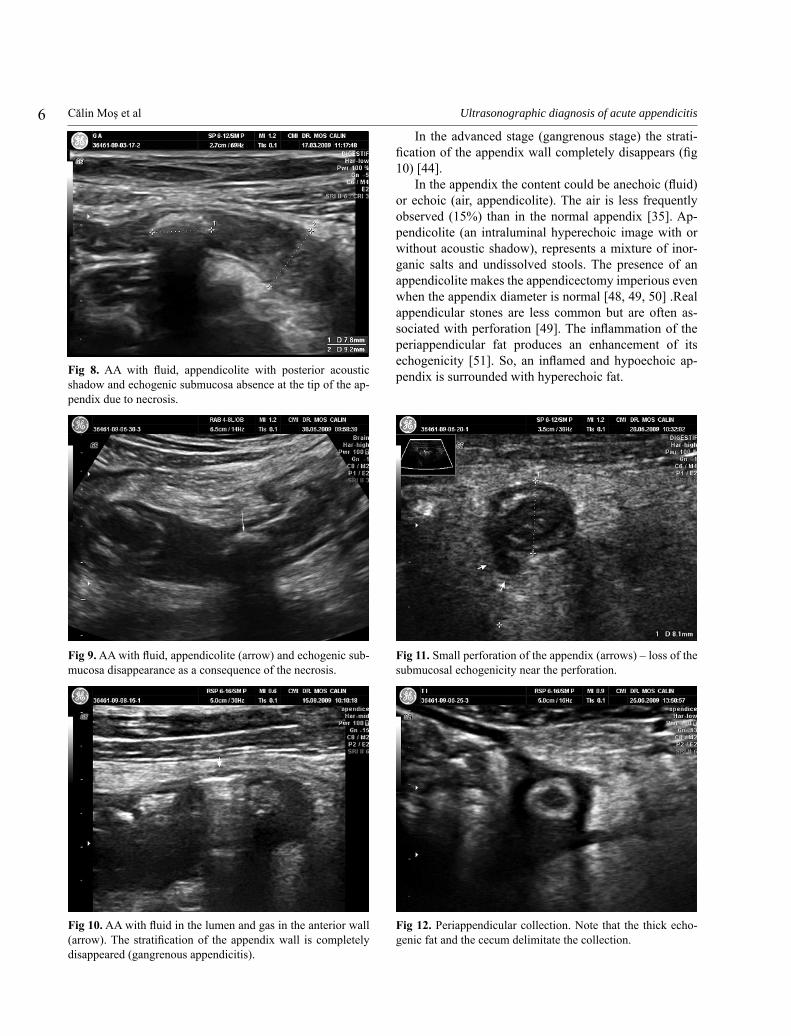
In the advanced stage (gangrenous stage) the strati-fi cation of the appendix wall completely disappears (fi g 10) [44].
In the appendix the content could be anechoic (fl uid) or echoic (air, appendicolite). The air is less frequently observed (15%) than in the normal appendix [35]. Ap-pendicolite (an intraluminal hyperechoic image with or without acoustic shadow), represents a mixture of inor-ganic salts and undissolved stools. The presence of an appendicolite makes the appendicectomy imperious even when the appendix diameter is normal [48, 49, 50] .Real appendicular stones are less common but are often as-sociated with perforation [49]. The infl ammation of the periappendicular fat produces an enhancement of its echogenicity [51]. So, an infl amed and hypoechoic ap-pendix is surrounded with hyperechoic fat. Fig 8. AA with fl uid, appendicolite with posterior acoustic
shadow and echogenic submucosa absence at the tip of the ap-pendix due to necrosis.
Fig 9. AA with fl uid, appendicolite (arrow) and echogenic sub-mucosa disappearance as a consequence of the necrosis.
Fig 10. AA with fl uid in the lumen and gas in the anterior wall (arrow). The stratifi cation of the appendix wall is completely disappeared (gangrenous appendicitis).
Fig 11. Small perforation of the appendix (arrows) – loss of the submucosal echogenicity near the perforation.
Fig 12. Periappendicular collection. Note that the thick echo-genic fat and the cecum delimitate the collection.

7Medical Ultrasonography 2009; 11(3): 7–18
Appendix perforation is suggested by the presence of a periappendicular collection (periappendicular abscess), submucosal discontinuity zones, asymmetric appendix walls thickening with possible intramural air, periappen-dicular fat thickening >10 mm (fi g 11, fi g 12, fi g 13).
Sometimes, there is no signifi cant pain during ex-amination (due to decreased pressure following appendix rupture) [47, 52]. The most specifi c feature is the pres-ence of the pericecal abscess, with impure fl uid content and small echoes inside and mass effect on the nearby intestinal ansae [52]. In small perforations, an emergency appendicectomy is necessary. In cases with periappendic-ular phlegmons, an initial conservative therapy followed by postponed appendicectomy is preferred. For well de-fi ned abscesses a US guided drainage can be performed before appendicectomy [52, 53, 54, 55, 56, 57].
In abortive appendicitis (7-10% of cases) the ap-pendix usually does not contains coprolites, no periap-pendicular abscess or infl ammatory signs are detected, and the average the appendix diameter is 8.5 mm [12, 13]. Recurrence rate after an abortive appendicitis is 38% after 3 months and 70% after 1 year. The recurrence is signifi cantly enhanced if the appendix diameter is >8 mm under compression [13].
The position of the appendix can infl uence its de-tection. A retrocecal appendix is better visualized from coronal sections (with the probe direction from lateral to medial). A pelvic appendix can be detecting by using an endovaginal probe. An unidentifi ed appendix is sugges-tive but not revealing for a normal appendix
In the differential diagnosis of AA, miscellaneous abdominal and extrabdominal pathology should be taken into account (tab IV).
In the last years, new techniques for the improvement of the US images have been used. In a recent study [58] the use of Spatial Compounding Imaging (cross beam) and Tissue Harmonic Imaging increased the rate of de-tection of the appendix by 19%.
The examiner’s experience in appendix US is very important. During this study the improvement in exam-iner’s abilities, especially for normal appendix identifi ca-tion, were recorded.
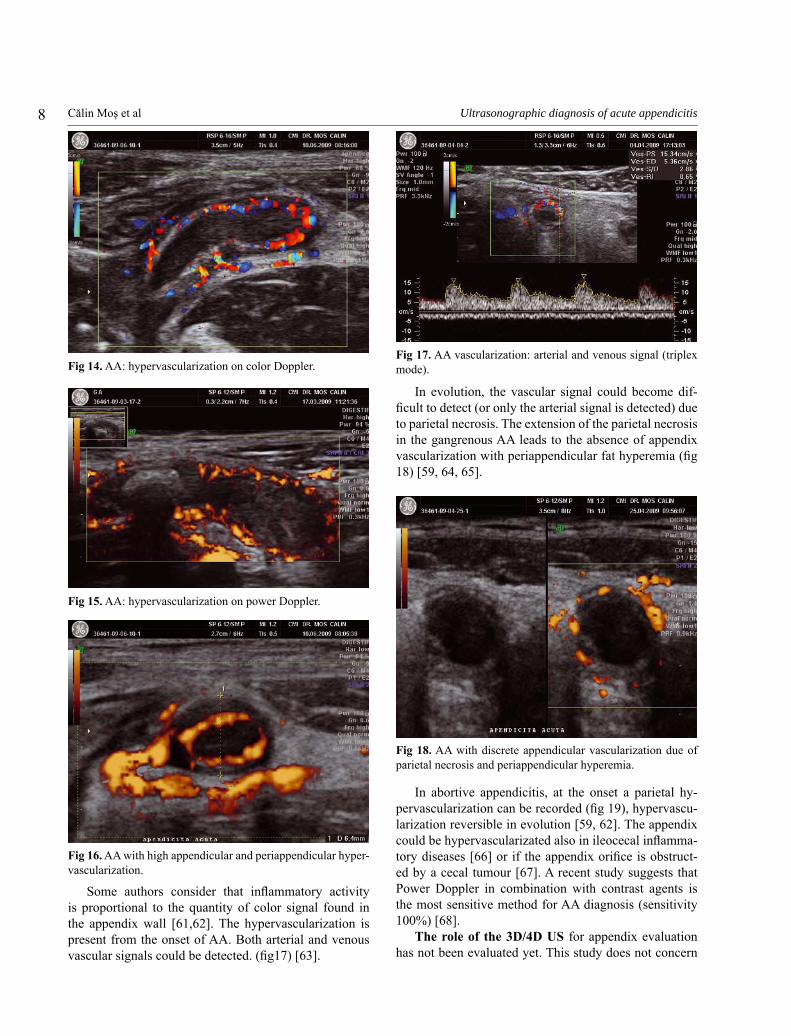
The normal appendicular vessels are of small cali-bres with slow blood velocities. The normal appendix does not usually present distinguishable vascularization at Doppler US. In AA the vascular diameters and blood velocities are increased, being easy to detect in Doppler US (fi g 14, fi g 15, fi g 16) [59, 60]
Fig 13. A diffuse collection in the right iliac fossa (periappen-dicular phlegmon).
Table IV. Differential diagnosis of the acute appendicitis
Differential diagnosis
Obstetrical and gynaecologic diseases Pelvic infl ammatory disease, ovarian cyst rupture, tubular pregnancy, tubular pathology, endometriosis
Gastrointestinal diseasesUlcer, diverticulitis, Chron’s disease, infectious enteritis, ileocecitis, ileitis, tuberculosis, intestinal occlusion, intestinal infarction, invagination, volvulus, tumors, acute pancreatitis, mesenteric adenitis, mesenteric infarction
Urinary diseases Renal colic, renal abscess, pyelonephritis, prostatitis testicular torsion
Liver and gallbladder diseases Hepatic abscess, acute cholecystitis
Muscle diseases Iliopsoas muscle abscess or haematoma, rectus abdominis muscle sheath haematoma
Epiploon diseases Infarction, torsion, appendagitis
Pulmonary diseases Pneumonia, pulmonary infarction
Parasitic infections Ascaridiosis
8 Călin Moş et al Ultrasonographic diagnosis of acute appendicitis
Some authors consider that infl ammatory activity is proportional to the quantity of color signal found in the appendix wall [61,62]. The hypervascularization is present from the onset of AA. Both arterial and venous vascular signals could be detected. (fi g17) [63].
In evolution, the vascular signal could become dif-fi cult to detect (or only the arterial signal is detected) due to parietal necrosis. The extension of the parietal necrosis in the gangrenous AA leads to the absence of appendix vascularization with periappendicular fat hyperemia (fi g 18) [59, 64, 65].
In abortive appendicitis, at the onset a parietal hy-pervascularization can be recorded (fi g 19), hypervascu-larization reversible in evolution [59, 62]. The appendix could be hypervascularizated also in ileocecal infl amma-tory diseases [66] or if the appendix orifi ce is obstruct-ed by a cecal tumour [67]. A recent study suggests that Power Doppler in combination with contrast agents is the most sensitive method for AA diagnosis (sensitivity 100%) [68].
The role of the 3D/4D US for appendix evaluation has not been evaluated yet. This study does not concern
Fig 14. AA: hypervascularization on color Doppler.
Fig 15. AA: hypervascularization on power Doppler.
Fig 16. AA with high appendicular and periappendicular hyper-vascularization.
Fig 17. AA vascularization: arterial and venous signal (triplex mode).
Fig 18. AA with discrete appendicular vascularization due of parietal necrosis and periappendicular hyperemia.
9Medical Ultrasonography 2009; 11(3): 7–18
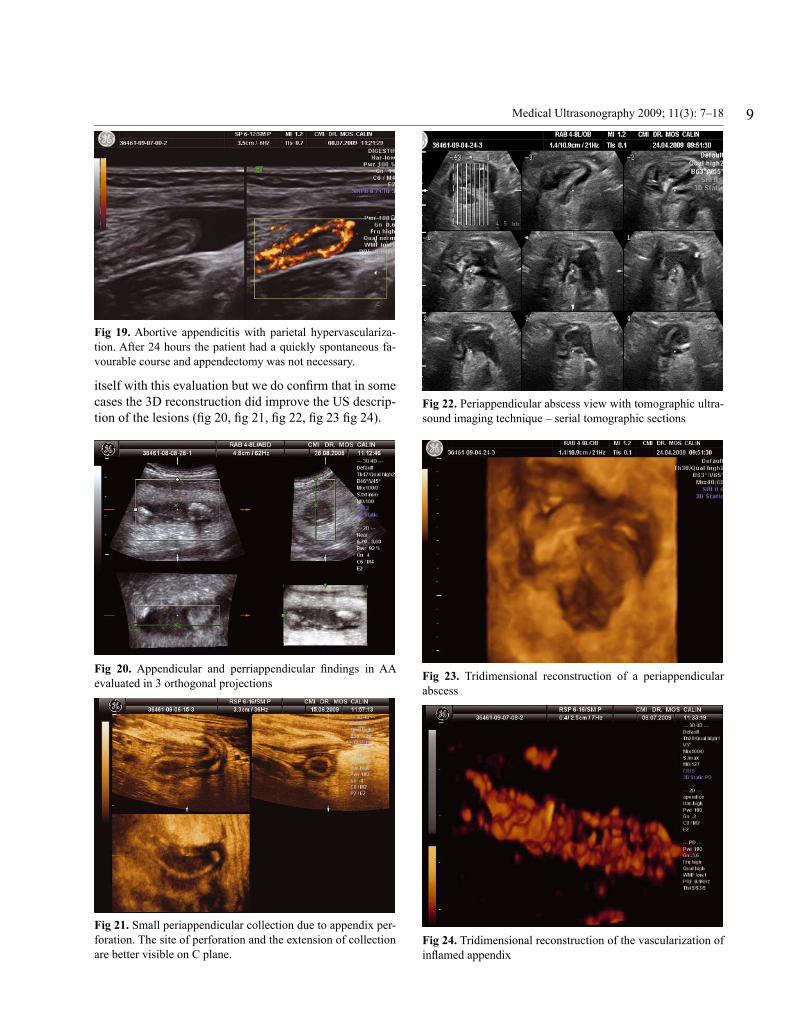
itself with this evaluation but we do confi rm that in some cases the 3D reconstruction did improve the US descrip-tion of the lesions (fi g 20, fi g 21, fi g 22, fi g 23 fi g 24).
Fig 19. Abortive appendicitis with parietal hypervasculariza-tion. After 24 hours the patient had a quickly spontaneous fa-vourable course and appendectomy was not necessary.
Fig 20. Appendicular and perriappendicular fi ndings in AA evaluated in 3 orthogonal projections
Fig 21. Small periappendicular collection due to appendix per-foration. The site of perforation and the extension of collection are better visible on C plane.
Fig 22. Periappendicular abscess view with tomographic ultra-sound imaging technique – serial tomographic sections
Fig 23. Tridimensional reconstruction of a periappendicular abscess
Fig 24. Tridimensional reconstruction of the vascularization of infl amed appendix

10 Călin Moş et al Ultrasonographic diagnosis of acute appendicitis
Our statistical analysis results are in concordance with those from the literature. The majority of studies showed a sensibility between 64-96%, specifi city be-tween 88-99%, accuracy between 82-97%, PPV between 79-99% and NPV between 75-97% of the US in AA diag-nosis [18, 25, 40, 60, 69, 70, 71, 72]. Our study confi rms that nowadays, with modern devices and an experienced operator, it is possible to achieve the most accurate re-sults.
The sensibility of the method was lower than the spe-cifi city because of the uncontrolled factors responsible for the majority of the false negative results (obesity, unspecifi c localization of appendix and associated dis-eases).
It must be mentioned that the US in our study was performed only after clinical examination and laboratory tests. The use of the US as a diagnostic method, together with clinical examination and laboratory tests decreased signifi cantly the rate of unnecessary appendicectomies from 20-30% [9, 10, 11, 70] to 9.9%.
Conclusion
Ultrasonography is a sensitive and specifi c method for AA diagnosis. In patients with right lower quadrant ab-dominal pain the US can identify the source of the pain- appendicular or non-appendicular. US has an important role in the AA management and also implications in the therapeutic decision. US examination could considerably decrease the number of unnecessary appendicectomies.
Acknowledgments
Special thanks to Mr. Sebastien Eckert, chairman of Medisys Societe, Paris, France for his priceless help.
References
1. Liu CD, McFadden DW. Acute abdomen and appendix. In: Greenfi eld LJ, et al., eds. Surgery: scientifi c principles and practice. 2d ed. Philadelphia: Lippincott-Raven, 1997: 1246-1261.
2. Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epide-miology of appendicitis and appendectomy in the United States. Am J Epidemiol 1990; 132: 910-925.
3. Schwartz SI. Appendix. In: Schwartz SI, ed. Principles of surgery. 6th ed. New York: McGraw Hill, 1994: 1307-1318.
4. Puig S, Hormann M, Rebhandl W, Felder-Puig RF, Prokop M, Paya K. US as a primary diagnostic tool in relation to negative appendectomy: six years experience. Radiology 2003; 226: 101–104.
5. Telford GL, Condon RE. Apendix. In: Zuidema GD, Sur-gery of the alimentary tract. 3rd ed. Philadelphia: Saunders, 1991: 133-141.
6. Hardin DM Jr. Acute appendicitis: review and update. Am Fam Physician 1999; 60: 2027-2034.
7. Wilcox RT, Traverso LW. Have the evaluation and treat-ment of acute appendicitis changed with new technology? Surg Clin North Am 1997; 77: 1355-1370.
8. Graffeo CS, Counselman FL. Appendicitis. Emerg Med Clin North Am 1996; 14: 653-671.
9. Deal DR. Acute appendicitis. In: Sleisonger MH, Fordtran JS, eds. Gastrointestinai disease. Pathophysiology, diag-nosis, management. Philadelphia:Saunders, 1973: 1494-1500.
10. Lewis FR, Holcroft JW, Boey J, Dunphy E. Appendicitis. A critical review of diagnosis and treatment in 1,000 cases. Arch Surg 1975; 110: 677-684.
11. Rao PM, Rhea JT, Novelline RA, Mostafavi AA, McCabe CJ. Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N Engl J Med 1998; 338: 141-146.
12. Migraine S, Atri M, Bret PM, Lough J0, Hinchey JE. Spon-taneously resolving acute appendicitis:clinical and sono-graphic documentation. Radiology 1997; 205: 55-58.
13. Cobben LP, de Van Otterloo AM, Puylaert JB. Spontane-ously resolving appendicitis: frequency and natural history in 60 patients. Radiology 2000; 215: 349–352.
14. Rao PM, Feltmate CM, Rhea JT, Schulick AH, Novelline RA. Helical computed tomography in differentiating ap-pendicitis and acute gynecologic conditions. Obstet Gyne-col 1999; 93: 417-421.
15. Rao PM, Rhea JT, Novelline RA, et al. Helical CT tech-nique for the diagnosis of appendicitis: prospective evalu-ation of a focused appendix CT examination. Radiology 1997; 202: 139-144.
16. Orr RK, Porter D, Hartman D. Ultrasonography to evalu-ate adults for appendicitis: decision making based on meta-analysis and probabilistic reasoning. Acad Emerg Med 1995; 2: 644-650.
17. Gaensler EH, Jeffrey RB Jr, Laing FC, Townsend RR. Sonography in patients with suspected acute appendici-tis: value in establishing alternative diagnoses. AJR Am J Roentgenol 1989; 152: 49-51.
18. Puylaert JB. Acute appendicitis: US evaluation using grad-ed compression. Radiology 1986; 158: 355-360.
19. Puylaert JB, Lalisang RI, van der Werf SD, Doornbos L. Campylobacter ileocolitis mimicking acute appendicitis: differentiation with graded-compression US. Radiology 1988; 166: 737–740.
20. Puylaert JB, Rutgers PH, Lalisang RI, et al. A prospective study of ultrasonography in the diagnosis of appendicitis. N Engl J Med 1987; 317: 666–669.
21. Garcia Pena BM, Mandl KD, Kraus SJ, et al. Ultrasonogra-phy and limited computed tomography in the diagnosis and management of appendicitis in children. JAMA 1999; 282: 1041–1046.
22. Schulte B, Beyer D, Kaiser C, Horsch S, Wiater A. Ultra-
11Medical Ultrasonography 2009; 11(3): 7–18
sonography in suspected acute appendicitis in childhood: report of 1285 cases. Eur J Ultrasound 1998; 8: 177–182.
23. Baldisserotto M, Marchiori E. Accuracy of noncompressive sonography of children with appendicitis according to the potential positions of the appendix. AJR Am J Roentgenol 2000; 175: 1387–1392.
24. Lee JH, Jeong YK, Hwang JC, Ham SY, Yang SO. Graded compression sonography with adjuvant use of a posterior manual compression technique in the sonographic diagno-sis of acute appendicitis. AJR Am J Roentgenol 2002; 178: 863-868.
25. Rioux M. Sonographic detection of the normal and abnor-mal appendix. AJR Am J Roentgenol 1992; 158: 773–778
26. Vriesman AB, Puylaert J. Appendix: mimics of appendi-citis. Alternative nonsurgical diagnoses at sonography and CT. The Radiology Assistant, 2005.
27. Lim HK, Lee WJ, Lee SJ, Namgung S, Lim JH. Focal ap-pendicitis confi ned to the tip: diagnosis at US. Radiology 1996; 200: 799–801.
28. Yabunaka K, Katsuda T, Sanada S, Fukutomi T. Sono-graphic appearance of the normal appendix in adults. J Ul-trasound Med 2007; 26: 37-43.
29. Jeffrey RB Jr, Laing FC, Lewis FR. Acute appendicitis: high-resolution real time US fi ndings. Radiology 1987; 163: 11-14.
30. Jeffrey RB Jr, Laing FC, Townsend RR. Acute appendicitis: sonographic criteria based on 250 cases. Radiology 1988; 167: 327–329.
31. Simonovsky V. Sonographic detection of normal and ab-normal appendix. Clin Radiol 1999; 54: 533–539.
32. Park NH, Park CS, Lee EJ, et al. Ultrasonographic fi ndings identifying the faecal-impacted appendix: differential fi nd-ings with acute appendicitis. Br J Radiol 2007; 80: 872-877.
33. Hahn HB, Hoepner FU, Kalle T, et al. Sonography of acute appendicitis in children: 7 years experience. Pediatr Radiol 1998; 28: 147–151.
34. Simonovsky V. Normal appendix: is there any signifi cant difference in the maximal mural thickness at us between pediatric and adult populations? Radiology 2002; 224: 333–337.
35. Rettenbacher T, Hollerweger A, Macheiner P, et al. Pres-ence or absence of gas in the appendix: additional criteria to rule out or confi rm acute appendicitis-evaluation with US. Radiology 2000; 214: 183-187.
36. Yabunaka K, Katsuda T, Sanada S, Fukutomi T. Sono-graphic appearance of the normal appendix in adults. J Ul-trasound Med 2007; 26: 37-43.
37. Rettenbacher T, Hollerweger A, Macheiner P, et al. Ovoid shape of the vermiform appendix: a criterion to exclude acute appendicitis – evaluation with US. Radiology 2003; 226: 95-100.
38. Fakhry JR, Berk RN. The “target” pattern: characteristic sonographic feature of stomach and bowel abnormalities. AJR Am J Roentgenol 1981; 137: 969-972.
39. Wiersma F, Sramek A, Holscher HC. US features of the normal appendix and surrounding area in children. Radiol-ogy 2005; 235: 1018-1022.
40. Abu-Yousef MM, Bleicher JJ, Maher JW, Urdaneta LF, Franken EA Jr, Metcalf AM. High-resolution sonography of acute appendicitis. AJR Am J Roentgenol 1987; 149: 53-58.
41. Deutsch A, Leopold GR. Ultrasonic demonstration of the infl amed appendix. Radiology 1981; 140: 163-164.
42. Himeno S, Yasuda S, Oida Y, et al. Ultrasonography for the diagnosis of acute appendicitis. Tokai J Exp Clin Med 2003; 28: 39-44.
43. Lee JH, Jeong YK, Park KB, Park JK, Jeong AK, Hwang JC. Operator-dependent techniques for graded compression sonography to detect the appendix and diagnose acute ap-pendicitis. AJR Am J Roentgenol 2005; 184: 91–97.
44. Takada T, Yasuda H, Uchiyama K, Hasegawa H, Shikata J. Ultrasonographic diagnosis of acute appendicitis in surgical indication. Int Surg 1986; 71 :9-13.
45. Jeffrey RB Jr, Laing FC, Lewis FR. Acute appendicitis: high-resolution real-time US fi ndings. Radiology 1987; 163: 11-14.
46. Sivit CJ, Siegel MJ, Applegate KE, Newman KD. When appendicitis is suspected in children. Radiographics 2001; 21: 247–262.
47. Borushok KF, Jeffrey RB Jr, Laing FC, Townsend RR. Sonographic diagnosis of perforation in patients with acute appendicitis. AJR Am J Roentgenol 1990; 154: 275-278.
48. Nitecki S, Karmeli R, Sarr MG.. Appendiceal calculi and fecaliths as indications for appendectomy. Surg Gynecol Obstet 1990; 171: 185–188.
49. Jones BA, Demetriades D, Segal I, Burkitt DP. The preva-lence of appendiceal fecaliths in patients with and without appendicitis: a comparative study from Canada and South Africa. Ann Surg 1985; 202: 80–82.
50. Shaw RE. Appendix calculi and acute appendicitis. Br J Surg 1965; 52: 451–459.
51. Noguchi T, Yoshimitsu K, Yoshida M. Periappendiceal hy-perechoic structure on sonography: a sign of severe appen-dicitis. J Ultrasound Med 2005; 24: 323–327.
52. Skoubo-Kristensen E, Hvid I. The appendiceal mass: con-servative management. Ann Surg 1982; 196: 584-587.
53. Hoffmann J, Lindhard A, Jensen HE. Appendix mass: con-servative management without interval appendectomy. Am J Surg 1984; 148: 379-382.
54. Bagi P, Dueholm S. Nonoperative management of the ultra-sonically evaluated appendiceal mass. Surgery 1987: 101: 602-605.
55. Paull DL, Bloom GP. Appendiceal abscess. Arch Surg 1982; 117: 1017-1019.
56. Jeffrey RB Jr, Tolentino CS, Federle MP, Laing FC. Percu-taneous drainage of periappendiceal abscesses: review of 20 patients. AJR Am J Roentgenol 1987; 149: 59-62.
57. Jeffrey RB Jr, Federle MP, Tolentino CS. Periappendiceal infl ammatory masses: CT-directed management and clini-cal outcome in 70 patients. Radiology 1988; 167: 13-16.
58. Scott T, Swan H, Jurriaans E, Voss M. Sonographic detec-tion of the normal appendix does the combination of real-time spatial compounding and tissue harmonic imaging make a difference? JDMS 2004; 20: 326-334.

12 Călin Moş et al Ultrasonographic diagnosis of acute appendicitis
59. Quillin SP, Siegel MJ. Appendicitis in children: color Dop-pler sonography. Radiology 1992; 184: 745-747.
60. Kessler N, Cyteval C, Gallix B, et al. Appendicitis: evalu-ation of sensiticity, specifi city and predictive values of US, Doppler US and laboratory fi ndings. Radiology 2004; 230: 472-478.
61. Lim HK, Lee WJ, Kim TH, Namgung S, Lee SJ, Lim JH. Appendicitis: usefulness of color Doppler US. Radiology 1996; 201: 221–225.
62. Quillin SP, Siegel MJ. Appendicitis: effi cacy of color Dop-pler sonography. Radiology 1994; 191: 557–560.
63. Patriquin HB, Garcier JM, Lafortune M, et al. Apendicitis in children and young adults: Doppler sonographic-pathologic correlation. AJR Am J Roentgenol 1996; 166: 629-633.
64. Quillin SP, Siegel MJ. Diagnosis of appendiceal abscess in children with acute appendicitis: value of color Doppler sonography. AJR Am J Roentgenol 1995; 164: 1251-1254.
65. Hernanz-Schulman M. Applications of Doppler sonogra-phy to diagnosis of extracranial pediatric disease. Radiol-ogy 1993; 189: 1-14.
66. Ripollés T, Martínez MJ, Morote V, Errando J. Appendiceal involvement in Crohn’s disease: gray-scale sonography and color Doppler fl ow features. AJR Am J Roentgenol
2006; 186: 1071–1078.67. Hermans JJ, Hermans AL, Risseeuw GA, Verhaar JC, Mer-
adji M. Appendicitis caused by carcinoid tumor. Radiology 1993; 188: 71-72.
68. Incesu L, Yazicioglu AK, Selcuk MB, Ozen N. Contrast-enhanced power Doppler US in the diagnosis of acute ap-pendicitis. Eur J Radiol 2004; 50: 201–209.
69. Hale DA, Molloy M, Pearl RH, Schutt DC, Jaques DP. Ap-pendectomy: a contemporary appraisal. Ann Surg 1997; 225: 252–261.
70. Riyad MN, Ouzounov GK, Wafaie IK, Gamal MA, Grover VK. Evaluation of sonography in the diagnosis of suspected acute apendicis. Kuwait Med J 2003; 33: 148-152.
71. Keyzer C, Zalcman M, De Maertelaer V, et al. Comparison of US and unenhanced multi-detector row CT in patients suspected of having acute appendicitis. Radiology 2005; 236: 527–534.
72. Doria AS, Moineddin R, Kellenberger CJ, et al. US or CT for diagnosis of appendicitis in children and adults? A meta-analysis? Radiology 2006; 241: 83-94.
73. Ooms HW, Koumans RK, Ho Kang You PJ, Puylaert JB. Ultrasonography in the diagnosis of acute appendicitis. Br J Surg 1991; 78: 315–318