tonsillar lymphoma masquerading as obstructive sleep … · case report tonsillar lymphoma...
TRANSCRIPT
Rom J Morphol Embryol 2016, 57(2 Suppl):885–891
ISSN (print) 1220–0522 ISSN (online) 2066–8279
CCAASSEE RREEPPOORRTT
Tonsillar lymphoma masquerading as obstructive sleep apnea – pediatric case report
CORNELIU TOADER1,2), MIORIŢA TOADER3), ALINA STOICA4), GABRIEL POP4), ALINA OPREA5), ANCA SIMONA CONSTANTIN6,7), LIVIU NICULESCU6,7), IOLANDA CRISTINA VIVISENCO5,8), MIRCEA STELIAN DRĂGHICI9), ANDREI OSMAN10), CARMEN AURELIA MOGOANTĂ10,11)
1)Department of Neurosurgery, National Institute of Neurology and Cerebrovascular Diseases, Bucharest, Romania 2)Department of Neurosurgery, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 3)Department of Otorhinolaryngology, “Grigore Alexandrescu” Clinical Emergency Hospital for Children, Bucharest, Romania
4)Department of Pathology, “Colentina” University Hospital, Bucharest, Romania 5)Department of Pediatrics, “Grigore Alexandrescu” Clinical Emergency Hospital for Children, Bucharest, Romania 6)Department of Pathology, “Grigore Alexandrescu” Clinical Emergency Hospital for Children, Bucharest, Romania 7)Department of Pathology, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 8)Department of Pediatrics, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 9)Dentirad Hospital, Ploieşti, Romania 10)Department of Otorhinolaryngology, Emergency County Hospital, Craiova, Romania 11)Department of Otorhinolaryngology, University of Medicine and Pharmacy of Craiova, Romania
Abstract The commonest cause of head and neck malignancy in pediatric patients is lymphoma. A particular case is the tonsillar lymphoma. Even though unilateral tonsillar enlargement represents an ominous sign for neoplasia, clinical manifestations vary and are non-specific. Therefore, a delayed diagnosis is performed which compromises optimal therapy and hinders the prognosis. We present the case of a 5-year-old boy who was initially diagnosed with obstructive sleep apnea, without reported systemic complaints. Asymmetric tonsillar hypertrophy created the premises for performing a tonsillectomy to rule out malignancy. The pathological evaluation of the resected tonsils revealed a malignant non-Hodgkin’s lymphoma, with immunophenotypic features consistent with sporadic type Burkitt lymphoma. The aim of this paper is to emphasize the importance of the histopathological examination and of the immunohistochemistry testing for the prompt and accurate diagnosis of all asymmetric tonsillar hypertrophy in children undergoing tonsillectomy. Furthermore, immunohistochemical diagnosis is vital for establishing a personalized multi-agent chemotherapy regimen, which dramatically improves the survival rate. We recommend histopathological evaluation in all children with asymmetric tonsillar hypertrophy undergoing tonsillectomy for various reasons. Needless to say, it is better to be cautious and exclude the presence of tonsillar lymphoma, than to confront with the severe consequences of misdiagnosis.
Keywords: Burkitt lymphoma, sporadic type, tonsillectomy, immunohistochemistry.
Introduction
Lymphoma represents the third most common pediatric neoplasia, the non-Hodgkin’s type being the most frequent. From a clinical standpoint, it consists of a chronic indurated cervical lymphadenopathy. 4–20% of patients with non-Hodgkin’s lymphoma present extra-nodal involvement in the head and neck, especially in the palatine tonsils. Actually, approximately 90% of lymphomas occur in the Waldeyer’s ring [1].
Extra-nodal localizations comprise initial presentation in the palatine tonsils, nasopharynx and the base of the tongue. Tonsils involvement produces a rapid asymmetric tonsillar hypertrophy, which leads to dysphagia, whereas involvement of the nasopharyngeal region produces hypo-nasal speech, persistent nasal obstruction and various forms of snoring [2]. In many cases, in the pediatric population, the described symptomatology is interpreted as obstructive sleep apnea, polysomnographic data certi-fying the diagnosis [3].
Even though unilateral tonsillar enlargement is an
ominous sign for neoplasia, clinical manifestations vary and are highly non-specific. As a result, the diagnosis of tonsillar lymphoma occurs late when the therapy becomes inefficient and creates the premises for a dismal prognosis. Needless to say, it is of paramount importance that practitioners are familiarized with the most frequent clinical manifestations of this pathology [4].
The two most frequent subgroups of non-Hodgkin’s lymphoma in children are the mature B-cell lymphomas, namely the Burkitt lymphoma and the diffuse large B-cell lymphoma. The first is a highly aggressive, potentially curable malignant tumor that is particularly sensitive to polychemotherapy, and notorious for its tumor lysis syndrome. It has a very short doubling time, thus the prompt diagnosis is crucial for the subsequent medical and eventually surgical treatment (World Health Organization – WHO) [5, 6].
We report a case of classic type sporadic Burkitt lymphoma developed in the tonsil of a 5-year-old boy presenting with obstructive sleep apnea due to asymmetric tonsillar enlargement. He received a bilateral palatine
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/

Corneliu Toader et al.
886
tonsillectomy in order to rule out a tonsillar malignancy and the pathologist’s report diagnosed a malignant non-Hodgkin’s lymphoma of the Burkitt type based on histo-pathological examination and immunohistochemistry tests.
Our aim is to outline the importance of establishing the clinical suspicion of tonsillar lymphoma in selected cases. In addition, we highlight the contribution of pathology studies to the prompt and accurate diagnosis of all asymmetric tonsillar hypertrophy in children undergoing tonsillectomy.
Case presentation
A 5-year-old boy was admitted on the Department of Pediatric Otolaryngology of “Grigore Alexandrescu” Clinical Emergency Hospital for Children, Bucharest, Romania, for snoring, nasal obstruction and hyponasal speech. The onset of the clinical complaints was three weeks prior admission with nasal obstruction accompanied by snoring, nocturnal mouth breathing, restlessness during sleep, and unusual sleeping positions. One week before, he associated nasal fonation. We mention that the child’s parents agreed with the report of the case and gave their informed consent for publication.
Past personal history revealed varicella and infectious mononucleosis at the age of three years. Physical exami-nation was normal except for adenoidal hypertrophy and grade II hypertrophy of left tonsilla. Laboratory tests were within normal range. A suspicion of obstructive sleep apnea was raised and a nocturnal polysomnography was recommended. Polysomnographic data showed light snore, with an apnea–hypopnea index of 7.07/h and average saturation of oxygen of 96% with a minimum saturation of 88%. After corroboration with the anamnesis and clinical data, the patient fulfilled the diagnostic criteria for the moderate form of pediatric obstructive sleep apnea.
Taking into the consideration that tonsillar asymmetry in the absence of acute infection is highly suspicious; the bilateral palatine tonsillectomy was recommended and eventually performed.
Materials and Methods
The resected specimens were sent to the Department of Pathology. They were measured and weighed fresh, and then sliced. The selected slices were taken for histological and immunohistochemical diagnosis. Those were fixed in 10% neutral buffered formalin for 24 hours, and then processed by paraffin embedding using the classical protocol with a fully enclosed tissue processor (Leica ASP200 S). The paraffin blocks were sectioned to produce 5 μm cups using a rotary microtome, and then transferred in a water bath (Fully Automated Rotary Microtome Leica RM2255). The cups were further collected onto slides and were stained using Hematoxylin–Eosin (HE).
For the immunohistochemistry study, the slides were initially dewaxed and hydrated. The antigen unmasking was performed by boiling the sections in a sodium citrate solution pH 6 for one minute in a pressure cooker (Novocastra™ Epitope Retrieval Solutions), and then rising them in cold tap water. The endogenous peroxidase activity was blocked by using 3–4% hydrogen peroxide solution (Novocastra™ Peroxidase Block) for 5 minutes, and then the slides were washed with 50 mM tris-buffered saline (TBS) solution pH 7.6 twice for 5 minutes. Next,
the slides were treated with a 0.4% casein solution in phosphate-buffered saline, with stabilizers, surfactant, and 0.2% Bronidox L as a preservative (Novocastra™ Protein Block) in order to reduce non-specific binding of primary and polymer.
At the end of this step, the slides were washed with the TBS solution twice for 5 minutes. After the application of the primary antibody reactive, a solution of rabbit anti-mouse IgG (<10 μg/mL) in 10% (v/v) animal serum in TBS/0.09% ProClin™ 950 (Novocastra™ Post Primary) was added for 30 minutes in order to detect the mouse antibody. At the end of this step, the slides were washed with the TBS solution twice for 5 minutes. The next step of the process relied on the use of a solution of anti-rabbit poly-HRP-IgG (<25 μg/mL) containing 10% (v/v) animal serum in TBS/0.09% ProClin™ 950 (Novolink™ Polymer). This was applied for 30 minutes to detect all the rabbit immunoglobulins, along with the post primary and all the rabbit primary antibodies that might have bound to the examined tissue. After the 30 minutes, the slides were washed with the TBS solution twice for five minutes. In the next step, the reaction of the substrate/ chromogen, 3,3’-diaminobenzidine (DAB) with the peroxi-dase produced a visible brown precipitate at the antigen site. This was prepared from a solution of DAB chromogen, 1.74% w/v 3,3’-diaminobenzidine, in a stabilizer solution (DAB Chromogen) and Novolink™ DAB Substrate Buffer, a buffered solution containing ≤0.1% hydrogen peroxide and preservative (Novolink™ Polymer). At the end of this reaction, the slides were washed with water and then, contrast was obtained using 0.1% Mayer’s Hematoxylin for counterstaining. They were then dehydrated using alcohol, clarified with xylene, and the coverslips were mounted using DPX medium (Fluka).
The immunohistochemistry was performed using the following antibodies: anti-CD20 (code NCL-L-CD20-L26, clone L26, 1:200 dilution, Novocastra, Germany), anti-CD68 (code NCL-L-CD68, clone 514H12, 1:100 dilution, Novocastra), anti-CD3 (code NCL-L-CD3-565, clone LN10, 1:500 dilution, Novocastra), anti-CD5 (code NCL-L-CD5-4C7, clone 4C7, 1:500 dilution, Novocastra), anti-Ki67 (code NCL-L-Ki67-MM1, clone MM1, 1:500 dilution, Novocastra). In addition, given the past personal history of the patient for infectious mononucleosis, we have also performed immunohistochemistry tests for Epstein–Barr virus (EBV) chronic infection (anti-EBV antibody). For antigen retrieval, we used heat-induced antigen retrieval on formalin-fixed, paraffin-embedded tissue sections (HIER) in pH 6.0 citrate buffer for 30 minutes, at 250C (Novocastra™ Epitope Retrieval Solutions). To visualize the reaction, we used NovoLink™ Polymer Detection System (Leica Biosystems, Germany). Three pathologists independently evaluated each slide.
Results
At gross examination, the left palatine tonsil was ovoid, measuring 1.3/1.1/0.9 cm and weighing 5.89 g, with a bosselated surface and a congestive cut surface. The right one was larger, ill-defined, measuring 1.7/1.5/1.1 cm, and weighing 7.69 g, with a fish flesh appearance and hemorrhagic areas.
Histologically, the right tonsil had an effaced follicular architecture due to a malignant lymphoid proliferation, which also diffusely infiltrated the neighboring connective
Tonsillar lymphoma masquerading as obstructive sleep apnea – pediatric case report
887
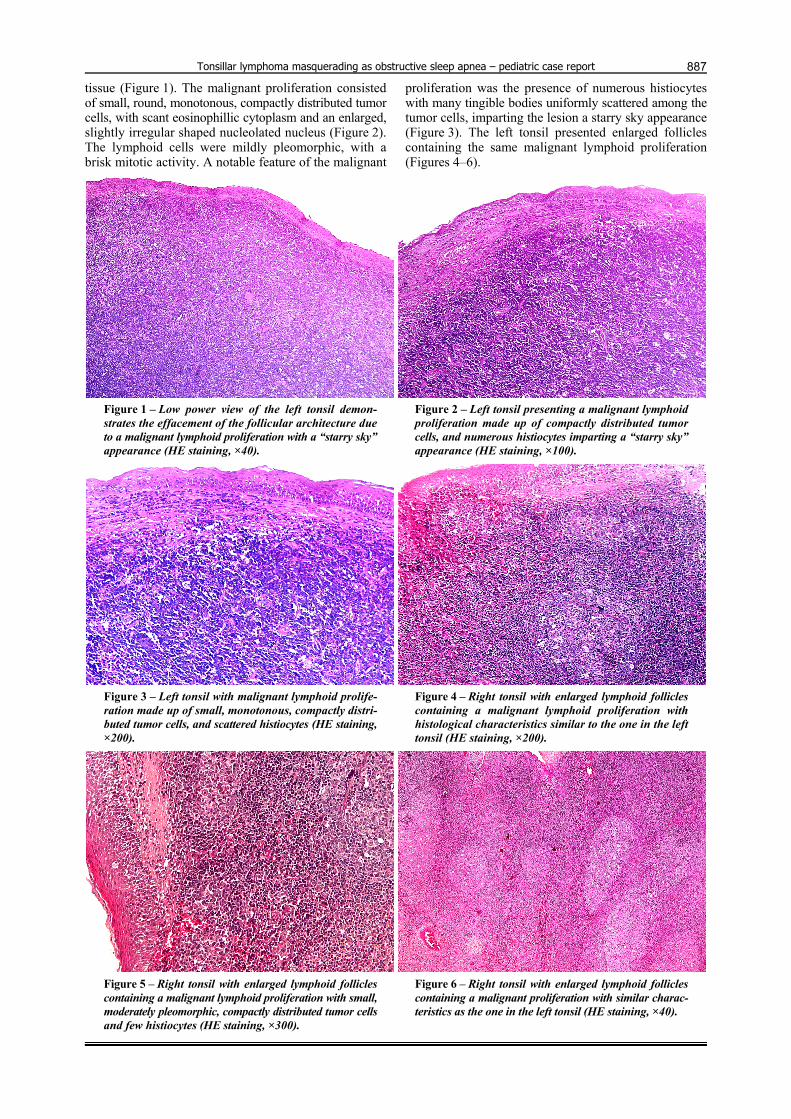
tissue (Figure 1). The malignant proliferation consisted of small, round, monotonous, compactly distributed tumor cells, with scant eosinophillic cytoplasm and an enlarged, slightly irregular shaped nucleolated nucleus (Figure 2). The lymphoid cells were mildly pleomorphic, with a brisk mitotic activity. A notable feature of the malignant
proliferation was the presence of numerous histiocytes with many tingible bodies uniformly scattered among the tumor cells, imparting the lesion a starry sky appearance (Figure 3). The left tonsil presented enlarged follicles containing the same malignant lymphoid proliferation (Figures 4–6).
Figure 1 – Low power view of the left tonsil demon-strates the effacement of the follicular architecture due to a malignant lymphoid proliferation with a “starry sky” appearance (HE staining, ×40).
Figure 2 – Left tonsil presenting a malignant lymphoid proliferation made up of compactly distributed tumor cells, and numerous histiocytes imparting a “starry sky” appearance (HE staining, ×100).
Figure 3 – Left tonsil with malignant lymphoid prolife-ration made up of small, monotonous, compactly distri-buted tumor cells, and scattered histiocytes (HE staining, ×200).
Figure 4 – Right tonsil with enlarged lymphoid follicles containing a malignant lymphoid proliferation with histological characteristics similar to the one in the left tonsil (HE staining, ×200).
Figure 5 – Right tonsil with enlarged lymphoid follicles containing a malignant lymphoid proliferation with small, moderately pleomorphic, compactly distributed tumor cells and few histiocytes (HE staining, ×300).
Figure 6 – Right tonsil with enlarged lymphoid follicles containing a malignant proliferation with similar charac-teristics as the one in the left tonsil (HE staining, ×40).
Corneliu Toader et al.
888
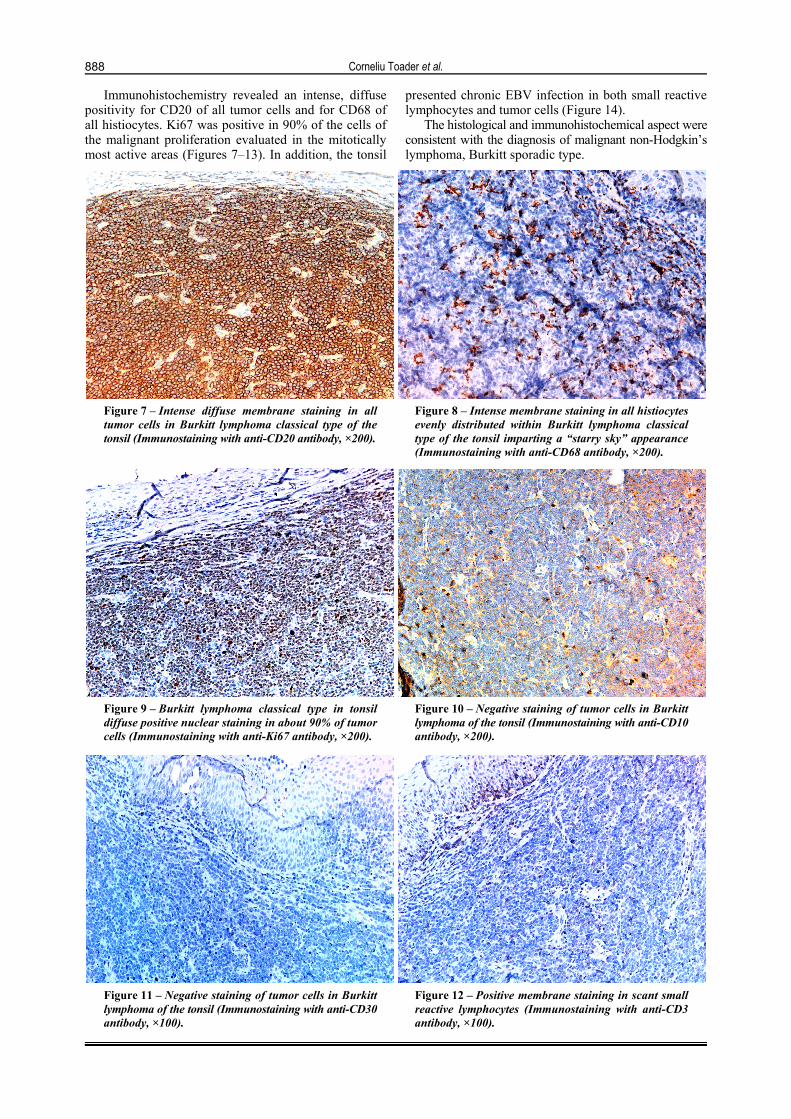
Immunohistochemistry revealed an intense, diffuse positivity for CD20 of all tumor cells and for CD68 of all histiocytes. Ki67 was positive in 90% of the cells of the malignant proliferation evaluated in the mitotically most active areas (Figures 7–13). In addition, the tonsil
presented chronic EBV infection in both small reactive lymphocytes and tumor cells (Figure 14).
The histological and immunohistochemical aspect were consistent with the diagnosis of malignant non-Hodgkin’s lymphoma, Burkitt sporadic type.
Figure 7 – Intense diffuse membrane staining in all tumor cells in Burkitt lymphoma classical type of the tonsil (Immunostaining with anti-CD20 antibody, ×200).
Figure 8 – Intense membrane staining in all histiocytes evenly distributed within Burkitt lymphoma classical type of the tonsil imparting a “starry sky” appearance (Immunostaining with anti-CD68 antibody, ×200).
Figure 9 – Burkitt lymphoma classical type in tonsil diffuse positive nuclear staining in about 90% of tumor cells (Immunostaining with anti-Ki67 antibody, ×200).
Figure 10 – Negative staining of tumor cells in Burkitt lymphoma of the tonsil (Immunostaining with anti-CD10 antibody, ×200).
Figure 11 – Negative staining of tumor cells in Burkitt lymphoma of the tonsil (Immunostaining with anti-CD30 antibody, ×100).
Figure 12 – Positive membrane staining in scant small reactive lymphocytes (Immunostaining with anti-CD3 antibody, ×100).

Tonsillar lymphoma masquerading as obstructive sleep apnea – pediatric case report
889
Figure 13 – Positive membrane staining in scant small reactive lymphocytes (Immunostaining with anti-CD5 antibody, ×200).
Figure 14 – Chronic EBV infection in lymphocytes of Burkitt lymphoma in tonsil (Immunostaining with anti-EBV antibody, ×200).
Discussion
Tonsillectomy is among the most common pediatric surgical routine procedures [7]. Is usually aimed at treating both malignant and non-neoplastic conditions such as recurrent infections, obstructive sleep apnea and severe snoring. However, because malignancy in grossly normal tonsils is an extremely rare pathological finding, throughout the world, some medical institutions prefer not to submit such resected specimens to the pathology department unless the surgeon explicitly requires their examination or a malignancy is suspected. Even more hospitals prefer to perform only the gross examination of the macroscopically normal tonsils, but such approaches are strictly forbidden in Romania, where all the resected specimens must be submitted to the department of pathology for macroscopic and microscopic examination [8].
Should some of those resected specimens not be submitted to the laboratory of pathology, or should they only be grossly examined, some malignancies may not be diagnosed in due time both in adult and in pediatric patients [8–10]. Tonsillectomy performed for a suspicion of malignancy is usually recommended for asymmetric tonsillar hypertrophy and ulceration [11]. Our patient presented with tonsillar asymmetry and the left tonsil was grossly modified, with subsequent malignant non-Hodgkin’s lymphoma, of the Burkitt type. What is interesting, although the right tonsil had a normal macroscopic appearance, its germinal centers were expanded and modified by the lymphoma.
Lymphoma involving the head and neck region in children is one of the most common pediatric malignancies. However, the tonsillar localization is rather rare for the non-Hodgkin’s type, occurring in 9% of the cases [8, 11]. Most of the patients present with a rapid onset of asymmetric tonsillar hypertrophy, which is highly suspicious and imposes tonsillectomy. Unfortunately, there is a consistent number of cases diagnosed only after the pathology report, some even after immunohistochemistry tests results [8, 12]. Taking into consideration the clinical manifestations, our patient was initially misdiagnosed with a moderate form of obstructive sleep apnea. However, the rapid evolution of the tonsillar hypertrophy and onset of symptoms raised the suspicion of malignancy. The
clinical assumptions were confirmed by the pathologist report. Therefore, we emphasize once more the importance of practitioners’ familiarization with clinical manifestations of tonsillar lymphoma. Furthermore, the tonsillectomy provided the frame for a timely and effective treatment.
The classic type sporadic Burkitt lymphoma is a rare malignancy usually seen in children, with boys being more frequently affected than girls (3:1 ratio) [1]. It presents with voluminous tumor masses that either compress onto or invade adjacent structures, but usually spare the lymph nodes [3, 4]. The cut section of the organ bearing it is somewhat sarcomatous. The microscopic appearance is of a population of monomorphous middle-sized monotonous malignant tumor cells, which efface the normal follicular appearance of the affected lymphoid tissue. Intermixed and uniformly distributed amongst them are normal histiocytes, which impart the characteristic “starry sky” appearance to the lymphoid proliferation. Their compact distribution renders them a somewhat cubical shape, their size being roughly the one of the nucleus of normal histiocytes. The tumor cells have a thin rim of basophilic cytoplasm and a large, slightly irregular, centrally located nucleus with several nucleoli and open chromatin. The Burkitt lymphoma has a very high mitotic index [5].
Along with the morphological features and the slight nuclear pleomorphism, the lymphoma was consistent with the classic immunophenotype of Burkitt subtype, thus respecting the main pathological key features. The specific immunophenotype characteristics consisted of positivity for pan-B-cell markers (CD20, CD79a, Pax5) and BCL6 strongly positive, BCL2 negative and Ki67 proliferation index greater than 90%. The staining for CD3 pan-T-cell marker only revealed rare admixed non-neoplastic small T-cells. The latter are usually described in most cases of diffuse large B-cell lymphoma [13]. Perhaps one of the greatest challenges for a pathologist is to pathologically differentiate Burkitt lymphoma from other types of non-Hodgkin’s lymphoma such as lymphoblastic lymphoma, blastoid mantle cell lymphoma (which mimics the appearance of lymphoblastic lymphoma) and diffuse large B-cell lymphoma [5, 14].
Both Burkitt and lymphoblastic lymphoma exhibit uniform cells with an intermediate nuclear size along

Corneliu Toader et al.
890
with an increased mitotic activity [14]. The distinctive morphologic features in lymphoblastic subtype are the leukemic pattern of infiltration and medium-sized cells with a scant cytoplasm and immature chromatin pattern with absent nucleoli [14, 15]. As for the immunopheno-type even though they share the BCL6 positive, the presence of the immaturity markers (TdT and CD34) is usually sufficient to exclude Burkitt lymphoma [13]. The blastoid mantle cell lymphoma present with medium-sized cells with irregular nuclei and absent nucleoli [15]. Markers for pan-B-cell are positive (CD19, CD20, CD22), but the presence of nuclear cyclin D1 along with CD5 establish the differential diagnosis. In addition, mantle cell lymphoma stains negative for CD10 and BCL6 [14]. Usually, diffuse large B-cell lymphoma are characterized by large-sized cells with irregular nuclei and no presence of “starry sky” pattern, which help to differentiate from Burkitt subtype [13]. However, in cases when overlapping morphological features are encountered, immunohisto-chemical staining for CD10 and BCL2 help establish the differential [14].
The patient presented with stage I classic Burkitt lymphoma as defined by Murphy classification, as a single extranodal site of involvement or the involvement of the lymph nodes within a single anatomic region, excepting the mediastinum and the abdomen. The treatment is based on chemotherapy, but debulking surgery for large tumor masses is helpful [10]. This patient received a bilateral tonsillectomy and vigorous chemotherapy according to the Anaplastic Large Cell Lymphoma (ALCL) 2000 Inter-national Protocol (including the administration of intra-thecal chemotherapy, given the potentially high-risk fir central nervous system relapse), which was well tolerated with minimum side effects. Needless to say, the immuno-histochemical diagnosis was of paramount importance for the establishment of a personalized multi-agent chemo-therapy regimen.
After therapy, he was longitudinally followed for the dreaded event of recurrences. Imaging studies consisting of PET/CT (positron emission tomography/computed tomography) scans were performed at periodic intervals, none showing signs of recurrence during the first two years of follow-up. Actually, relapse, if it does occur, it is predominantly encountered in the first 12 months after diagnosis [6]. Disrespectful of its highly aggressive nature, Burkitt lymphoma is a potentially curable lymphoma. It benefits from a superior prognosis when the diagnosis is established in a limited-stage and when it affects the pediatric population [13]. For the patient presented, taking into account all the disease’s features (clinical and patho-logical) the five-year survival rate is greater than 90%.
As far as the identified tonsillar chronic infection with EBV is concerned, EBV is not regarded as a causative agent for the development of Burkitt lymphoma. It causes a chronic infection by colonizing the B-lymphocytes memory cells [16, 17]. Besides producing the infectious mononucleosis, is linked to Burkitt lymphoma, Hodgkin’s lymphoma and nasal NK-/T-lymphoma, along with gastric adenocarcinoma and nasopharyngeal carcinoma [18, 19]. On this ground, the EBV is classified by the WHO as a carcinogen. The genome of the EBV has been thoroughly analyzed in an attempt to clarify its participation in the
pathogenesis of those malignancies. It has been recom-mended that all pediatric patients diagnosed with infectious mononucleosis shall be screened both by physical exa-mination and laboratory tests in order to identify one of the above mentioned lymphoid malignancies from their initial phase [20].
Infectious mononucleosis in children is not uncommon, the disease being a notorious manifestation of the EBV infection. The pathogen has a propensity to induce lymphomas when the host has an immunodeficiency and the appropriate strand of the virus. However, there are few reported cases of Burkitt lymphoma with positive Paul–Bunnel–Davidson reaction in children [11, 21]. In this case report, the patient was diagnosed with infectious mononucleosis at the age of three, when the infection is usually clinically unapparent. Regardless of the acute manifestation, the infection is chronic, whether or not the patient suffers from an underlying immunodeficiency. It has the ability of infecting not only B-cells but also T-cells, NK-cells and even epithelial cells [22]. The infection in the oropharynx is followed by infection of circulating B-cells leading to persistence of the viral DNA as an episome in the nucleus [23]. The lymphoma develops after a period of polyclonal activation of the B-lymphocytes infected with the EBV, in the setting of an inefficient T-lymphocyte modulation [11].
Conclusions
Establishing a prompt diagnosis for pediatric tonsillar lymphoma is vital for improving the long-term prognosis. Asymmetric tonsillar hypertrophy should be regarded as a suspicious sign for malignancy and on no account should it be ignored. Histological analysis of resected tonsils should be performed whenever the clinical setting is suggestive for an underlying potential neoplasia. Immuno-histochemical staining is of paramount importance, not only for certifying the diagnosis of Burkitt lymphoma but also for performing the differential diagnosis with other B-cell lymphoproliferative disorders. The described immunophenotype will guide the clinician towards the best option of a personalized chemotherapy regimen.
Conflict of interests The authors declare that they have no conflict of
interests to disclose.
References [1] Guimarães AC, de Carvalho GM, Bento LR, Correa C,
Gusmão RJ. Clinical manifestations in children with tonsillar lymphoma: a systematic review. Crit Rev Oncol Hematol, 2014, 90(2):146–151.
[2] Gaini RM, Romagnoli M, Sala A, Garavello W. Lymphomas of head and neck in pediatric patients. Int J Pediatr Oto-rhinolaryngol, 2009, 73(Suppl 1):S65–S70.
[3] Abdel-Aziz M, Ibrahim N, Ahmed A, El-Hamamsy M, Abdel-Khalik MI, El-Hoshy H. Lingual tonsils hypertrophy; a cause of obstructive sleep apnea in children after adenotonsillectomy: operative problems and management. Int J Pediatr Otorhino-laryngol, 2011, 75(9):1127–1131.
[4] Dolev Y, Daniel SJ. The presence of unilateral tonsillar enlargement in patients diagnosed with palatine tonsil lymphoma: experience at a tertiary care pediatric hospital. Int J Pediatr Otorhinolaryngol, 2008, 72(1):9–12.
[5] Freedman AS, Aster JC. Epidemiology, clinical manifestations, pathologic features, and diagnosis of Burkitt lymphoma. UpToDate, March 2014.

Tonsillar lymphoma masquerading as obstructive sleep apnea – pediatric case report
891
[6] Diebold J, Jaffe ES, Raphael M, Warnke RA. Burkitt lymphoma. In: Jaffe ES, Harris NL, Stein H, Vardiman JW (eds). Pathology and genetics of tumours of haematopoietic and lymphoid tissues. World Health Organization (WHO) Classification of Tumours, IARC Press, Lyon, 2001, 181–185.
[7] Verma SP, Stoddard T, Gonzalez-Gomez I, Koempel JA. Histologic analysis of pediatric tonsil and adenoid specimens: is it really necessary? Int J Pediatr Otorhinolaryngol, 2009, 73(4):547–550.
[8] Booth CL, Wang J. Occult hematologic malignancy in routine tonsillectomy specimens: a single institutional experience and review of the literature. Am J Clin Pathol, 2013, 140(6):807–812.
[9] Randall DA, Martin PJ, Thompson LDR. Routine histologic examination is unnecessary for tonsillectomy or adenoid-ectomy. Laryngoscope, 2007, 117(9):1600–1604.
[10] Zarbo RJ, Nakhleh RE. Surgical pathology specimens for gross examination only and exempt from submission: a College of American Pathologists Q-Probes study of current policies in 413 institutions. Arch Pathol Lab Med, 1999, 123(2):133–139.
[11] Sayed K, Van Savell H Jr, Hutchison RE, Kepner J, Link MP, Schwenn M, Mahmoud H, Parham DM. Review of tonsillar lymphoma in pediatric patients from the pediatric oncology group: what can be learned about some indications for microscopic examination? Pediatr Dev Pathol, 2005, 8(5): 533–540.
[12] Cunningham MJ, Myers EN, Bluestone CD. Malignant tumors of the head and neck in children: a twenty-year review. Int J Pediatr Otorhinolaryngol, 1987, 13(3):279–292.
[13] Sohani AR, Hasserjian RP. Diagnosis of Burkitt lymphoma and related high-grade B-cell neoplasms. Surg Pathol Clin, 2010, 3(4):1035–1059.
[14] Gascoyne RD, Siebert R, Connors JM. Chapter 24: Burkitt’s lymphoma. In: Jaffe ES, Lee Harris N, Vardiman JW, Campo E,
Arber DA (eds). Hematopathology. 1st edition, Elsevier–Saunders, 2011, 391–409.e5.
[15] O’Malley DP, Grimm KE, Banks PM. Chapter 6: Immuno-histology of non-Hodgkin lymphoma. In: Dabbs DJ (ed). Diagnostic immunohistochemistry: theranostic and genomic applications. 4th edition, Elsevier–Saunders, 2014, 148–188.e5.
[16] Luzuriaga K, Sullivan JL. Infectious mononucleosis. N Engl J Med, 2010, 362(21):1993–2000.
[17] Vetsika EK, Callan M. Infectious mononucleosis and Epstein–Barr virus. Expert Rev Mol Med, 2004, 6(23):1–16.
[18] Rickinson AB, Kieff ED. Epstein–Barr virus. In: Knipe DM, Howley PM, Griffin DE, Lamb RA, Martin MA, Roizman B, Straus SE (eds). Fields virology. 5th edition, Lippincott Williams & Wilkins, Wolters Kluwer, Philadelphia, PA, 2007, 2655–2700.
[19] Young LS, Rickinson AB. Epstein–Barr virus: 40 years on. Nat Rev Cancer, 2004, 4(10):757–768.
[20] Lorenzetti MA, Gantuz M, Altcheh J, De Matteo E, Chabay PA, Preciado MV. Distinctive Epstein–Barr virus variants associated with benign and malignant pediatric pathologies: LMP1 sequence characterization and linkage with other viral gene polymorphisms. J Clin Microbiol, 2012, 50(3):609–618.
[21] Noorbakhsh S, Siadati A, Ashtiani F, Mamishi S, Kooh Paiezadeh S. Comparative study of specific EBV antibodies between children manifest classic triad of mononucleosis with unaffected children in Hazrat Rasool Akram Hospital (1998–2000). Iran J Allergy Asthma Immunol, 2003, 2(2):81–88.
[22] Auerbach A, Aguilera NS. Epstein–Barr virus (EBV)-associated lymphoid lesions of the head and neck. Semin Diagn Pathol, 2015, 32(1):12–22.
[23] Rezk SA, Weiss LM. Epstein-Barr virus-associated lympho-proliferative disorders. Hum Pathol, 2007, 38(9):1293–1304.
Corresponding author Mioriţa Toader, MD, PhD, Pediatric Otolaryngologist, Department of Otorhinolaryngology, “Grigore Alexandrescu” Clinical Emergency Hospital for Children, 30–32 Iancu de Hunedoara Avenue, Sector 1, 011743 Bucharest, Romania; Phone +4021–316 93 66, e-mail: [email protected] Received: October 30, 2015
Accepted: November 4, 2016