doliul
DESCRIPTION
DoliulTRANSCRIPT

INTRODUCTION:
What is bereavement?
Bereavement, or grief, is defined as a set of reactions to a significant loss. While bereavement usually refers to the loss of a loved one, it may also refer to the loss of employment, a physical ability, possessions, or other events.
Bereavement is a word used to denote grief, pain and sadness following the loss of a loved one. Even though death is an inevitable part of life, the finality and irrevocability of death lends a lethal blow, making it ‘unacceptable’ for those left behind. It is truly one of life’s most stressful periods, with nothing to match the intensity of sorrow experienced during this time.
Bereavement is a complex process that is considered normal and may be accompanied by a variety of emotional reactions, behavioral responses, and thoughts. For example, in the course of bereavement you may experience sadness, anger, or relief. You may also feel the urge to withdraw from other people or to seek out social support.
Bereavement that is prolonged, overwhelming, or seriously impairing may be considered "complicated bereavement," a condition that may require intervention.
Bereavement is also a time of overwhelming and conflicting emotions. What may begin as shock and disbelief may give way to reflection, realization and acceptance as time passes by. Physical signs of bereavement may be portrayed as crying, expressing anger, loss of appetite, dip in energy levels and even sleeplessness. Psychological signs could be depression, feeling lost, being aloof or withdrawn, guilt and even anger.
Frequently reported symptoms in the first year of bereavement were sleep problems, nervous tension, depression, loss of appetite and pain. Mental health status and caregivers relational status were strong predictors of poor adjustment in early bereavement. Other risk factors included female gender, older age, grief in the past and emotional burden.
Understand that other family members may not feel these mixed emotions that you harbor. Do not use the immediate death or funeral to speak unkindly of him or her. Others might be grieving grandparents intensely and your negative words will not be taken well. Let the time of death and months afterward be a time for mourning even if you cannot participate. If your unresolved issues you hold continue to bother you, do not hesitate to
seek the counsel of a therapist or clergy member. Talking about these issues and dealing with them may be just what you need for healing.
In an ideal world, every death is a sad one and longing for and missing the deceased is a constant. However, in a realist world, sometimes there have been problems with your loved ones and their death may complicate feelings or issues you held. Perhaps your relationship with the deceased was not a happy one. Questions went unanswered or there was a sticky situation regarding the Will. At the time of the death of your grandparent, respect who he or she was as much as you can.
Support from loved ones, caring, talking ones grief out and even seeking professional help are ways to cope with the bereavement.
Several studies indicate that the majority of caregivers adjust reasonably well after the death of the person they cared for. Studies indicate that caregivers report a range of feelings in bereavement including loneliness, sadness, apathy, relief and overwhelming feelings of being back in the situation.
Definition
Bereavement refers to the period of mourning and grief following the death of a beloved person or animal. The English word bereavement comes from an ancient Germanic root word meaning "to rob" or "to seize by violence." Mourning is the word that is used to describe the public rituals or symbols of bereavement, such as holding funeral services, wearing black clothing, closing a place of business temporarily, or lowering a flag to half mast. Grief refers to one's personal experience of loss; it includes physical symptoms as well as emotional and spiritual reactions to the loss. While public expressions of mourning are usually time-limited, grief is a process that takes most people several months or years to work through.
Causes of Bereavements
The immediate cause of bereavement is usually the death of a loved friend or relative. There are a number of situations, however, which can affect or prolong the grief process:
• The relationship with the dead person was a source of pain rather than love and support. Examples would include an abusive parent or spouse.
• The person died in military service or in a natural, transportation, or workplace disaster. Bereavement in these cases is often made more difficult by intrusive news reporters as well as anxiety over the loved one's possible physical or mental suffering prior to death.

• The person was murdered. Survivors of homicide victims often find the criminal justice system as well as the media frustrating and upsetting.
• The person is missing and presumed dead but their death has not been verified. As a result, friends and relatives may alternate between grief and hope that the person is still alive.
• The person committed suicide. Survivors may feel guilt over their inability to foresee or prevent the suicide, shame that the death was self-inflicted, or anger at the person who committed suicide.
• The relationship with the dead person cannot be openly acknowledged. This situation often leads to what is called disenfranchised grief. The most common instances are homosexual or extramarital sexual relationships that have been kept secret for the sake of spouses or other family members.
• The loved one was an animal rather than a human being. Western societies are only beginning to accept that adults as well as children can grieve for a dead animal; many adults still feel that there is "something wrong" about grieving for their pet. The question of euthanasia may be an additional source of sorrow; even when the pet is terminally ill, many people are very uneasy about making the decision to end its life.
Symptoms of Bereavement
Bereavement typically affects a person's physical well-being as well as emotions. Common symptoms of grief include changes in appetite and weight, fatigue, insomnia and other sleep disturbances, loss of interest in sex, low energy levels, nausea and vomiting, chest or throat pain, and headache. People who have lost a loved one in traumatic circumstances may have such symptoms of post-traumatic stress disorder as an exaggerated startle response, visual or auditory hallucinations, or high levels of muscular tension.
• Physical pain - tightness in the body, breathlessness, lack of energy• Confusion, hallucinations, disbelief• Obsession with the deceased, sleeplessness, lack of appetite
Doctors and other counselors have identified four stages or phases in uncomplicated bereavement:

• Shock, disbelief, feelings of numbness. This initial phase lasts about two weeks, during which the bereaved person finally accepts the reality of the loved one's death.
• Suffering the pain of grief. This phase typically lasts for several months. Some people undergo a mild temporary depression about six months after the loved one's death.
• Adjusting to life without the loved one. In this phase of bereavement, survivors may find themselves taking on the loved one's roles and responsibilities as well as redefining their own identities.
Moving forward with life, forming new relation-ships, and having positive expectations of the future. Most people reach this stage within one to two years after the loved one's death.
What issues can Bereavement Counseling address?
• It can offer an understanding of the mourning process• To explore areas which might restrict moving on such as child abuse• Help resolve areas of conflict still remaining• Help to adjust to a new sense of self• Consider if the mourning has turned to depression
Talking about the loss is usually helpful and allows a person to adjust to their new life with all its changes, good and bad. Keeping things bottled up, or denying the sadness can prolong the pain.
Any loss has to be acknowledged for us to move forward. Bereavement means finding a suitable place for the lost person to allow life to continue with adaptation and change, not forgetting or wiping out the memory.
Description :Bereavement is a highly individual as well as a complex experience. It is
increasingly recognized that no two people respond the same way to the losses associated with the death of a loved one. People's reactions to a death are influenced by such factors as ethnic or religious traditions; personal beliefs about life after death; the type of relationship ended by death (relative, friend, colleague, etc.); the cause of death; the person's age at death; whether the death was sudden or expected; and many others. In addition, the death of a loved one inevitably confronts adults (and older adolescents) with the fact that they too will die. As a result of this variety and emotional complexity, most

doctors and other counselors advise people to trust their own feelings about bereavement, 0 and grieve in the way that seems most helpful to them.
It is also increasingly understood in the early 2000s that people can experience bereavement with regard to other losses. Some examples of these so-called "silent losses" include miscarriages in early pregnancy, the death of a child in the womb shortly before birth, or the news that a loved one has Alzheimer's disease or another illness that slowly destroys their personality. In addition, many counselors recognize that bereavement has two dimensions, the actual loss and the symbolic losses. For example, a person whose teenage son or daughter is killed in an accident suffers a series of symbolic losses—knowing that their child will never graduate from high school, get married, or have children—as well as the actual loss of the adolescent to death.
Coping With LossBereavement, or grief, is defined as a set of reactions to a significant loss. While
bereavement usually refers to the loss of a loved one, it may also refer to the loss of employment, a physical ability, possessions, or other events.
The loss of a loved one is life’s most stressful event and can cause a major emotional crisis. After the death of someone you love, you experience bereavement, which literally means “to be deprived by death.”
Bereavement - Consequences
When a death takes place, you may experience a wide range of emotions, even when the death is expected. Many people report feeling an initial stage of numbness after first learning of a death, but there is no real order to the grieving process.
Some emotions you may experience include:
• Denial • Disbelief • Confusion • Shock • Sadness • Yearning • Anger • Humiliation • Despair • Guilt

These feelings are normal and common reactions to loss. You may not be prepared for the intensity and duration of your emotions or how swiftly your moods may change. You may even begin to doubt the stability of your mental health. But be assured that these feelings are healthy and appropriate and will help you come to terms with your loss.
• Mourning A Loved One
It is not easy to cope after a loved one dies. You will mourn and grieve. Mourning is the natural process you go through to accept a major loss. Mourning may include religious traditions honoring the dead or gathering with friends and family to share your loss. Mourning is personal and may last months or years.
Grieving is the outward expression of your loss. Your grief is likely to be expressed physically, emotionally, and psychologically. For instance, crying is a physical expression, while depression is a psychological expression.
It is very important to allow yourself to express these feelings. Often, death is a subject that is avoided, ignored or denied. At first it may seem helpful to separate yourself from the pain, but you cannot avoid grieving forever. Someday those feelings will need to be resolved or they may cause physical or emotional illness.
Many people report physical symptoms that accompany grief. Stomach pain, loss of appetite, intestinal upsets, sleep disturbances and loss of energy are all common symptoms of acute grief. Of all life’s stresses, mourning can seriously test your natural defense systems. Existing illnesses may worsen or new conditions may develop.
Profound emotional reactions may occur. These reactions include anxiety attacks, chronic fatigue, depression and thoughts of suicide. An obsession with the deceased is also a common reaction to death.
Dealing with a Major Loss of Bereavement
The death of a loved one is always difficult. Your reactions are influenced by the circumstances of a death, particularly when it is sudden or accidental. Your reactions are also influenced by your relationship with the person who died.
A child’s death arouses an overwhelming sense of injustice — for lost potential, unfulfilled dreams and senseless suffering. Parents may feel responsible for the child’s

death, no matter how irrational that may seem. Parents may also feel that they have lost a vital part of their own identity.
A spouse’s death is very traumatic. In addition to the severe emotional shock, the death may cause a potential financial crisis if the spouse was the family’s main income source. The death may necessitate major social adjustments requiring the surviving spouse to parent alone, adjust to single life and maybe even return to work.
Elderly people may be especially vulnerable when they lose a spouse because it means losing a lifetime of shared experiences. At this time, feelings of loneliness may be compounded by the death of close friends.
A loss due to suicide can be among the most difficult losses to bear. They may leave the survivors with a tremendous burden of guilt, anger and shame. Survivors may even feel responsible for the death. Seeking counseling during the first weeks after the suicide is particularly beneficial and advisable.
How to cope up with Bereavement ?
Coping with death is vital to your mental health. It is only natural to experience grief when a loved one dies. The best thing you can do is allow yourself to grieve. There are many ways to cope effectively with your pain.
• Seek out caring people. Find relatives and friends who can understand your feelings of loss. Join support groups with others who are experiencing similar losses.
• Express your feelings. Tell others how you are feeling; it will help you to work through the grieving process.
• Take care of your health. Maintain regular contact with your family physician and be sure to eat well and get plenty of rest. Be aware of the danger of developing a dependence on medication or alcohol to deal with your grief.
• Accept that life is for the living. It takes effort to begin to live again in the present and not dwell on the past.
• Postpone major life changes. Try to hold off on making any major changes, such as moving, remarrying, changing jobs or having another child. You should give yourself time to adjust to your loss.
• Be patient. It can take months or even years to absorb a major loss and accept your changed life.
• Seek outside help when necessary. If your grief seems like it is too much to bear, seek professional assistance to help work through your grief. It’s a sign of strength, not weakness, to seek help.

Helping Others Grieve
If someone you care about has lost a loved one, you can help them through the grieving process.
• Share the sorrow. Allow them — even encourage them — to talk about their feelings of loss and share memories of the deceased.
• Don’t offer false comfort. It doesn’t help the grieving person when you say “it was for the best” or “you’ll get over it in time.” Instead, offer a simple expression of sorrow and take time to listen.
• Offer practical help. Baby-sitting, cooking and running errands are all ways to help someone who is in the midst of grieving.
• Be patient. Remember that it can take a long time to recover from a major loss. Make yourself available to talk.
• Encourage professional help when necessary. Don’t hesitate to recommend professional help when you feel someone is experiencing too much pain to cope alone.
Helping Children Grieve
Children who experience a major loss may grieve differently than adults. A parent’s death can be particularly difficult for small children, affecting their sense of security or survival. Often, they are confused about the changes they see taking place around them, particularly if well-meaning adults try to protect them from the truth or from their surviving parent’s display of grief.
Limited understanding and an inability to express feelings puts very young children at a special disadvantage. Young children may revert to earlier behaviors (such as bed-wetting), ask questions about the deceased that seem insensitive, invent games about dying or pretend that the death never happened.
Coping with a child’s grief puts added strain on a bereaved parent. However, angry outbursts or criticism only deepen a child’s anxiety and delays recovery. Instead, talk honestly with children, in terms they can understand. Take extra time to talk with them about death and the person who has died. Help them work through their feelings and remember that they are looking to adults for suitable behavior.

Support for the primary caregiver and family
P. Hudson and Payne (2009b) have outlined several reasons why governments and health and social care agencies should offer support to family caregivers:
caregivers are profoundly affected by the patient’s terminal illness
caregivers are responsible for numerous tasks
caregivers are prone to physical and psychological morbidity
caregivers are financially disadvantaged
caregivers have limited exposure to death and dying
caregivers are pivotal in achieving „successful‟ home care
caregivers are often excluded from information and care planning
caregivers can become socially isolated
caregivers commonly report unmet needs.
The World Health Organization (WHO) advocates that palliative care should improve the quality of life of patients and their families facing problems associated with terminal illness (World Health Organization, 2002).
Palliative care services are ideally placed to provide support to caregivers and family members of terminally ill patients. Service providers are often in close contact with families and have the opportunity to build rapport and trust over a period of time. The potential benefit of obtaining support from a specialist palliative care program was shown in a US cohort study whereby 30,838 elderly couples were retrospectively matched on the basis of whether or not the decedent was the recipient of hospice care. Findings showed that the surviving spouse of decedents who received hospice care were less likely to fall ill and die during bereavement than spouses of decedents who did not receive hospice care (Christakis & Iwashyna, 2003).
Within Australian health policy standards it is explicitly acknowledged that the needs of primary caregivers and family members should be considered as an integral component in the provision of specialist palliative care services (P. Hudson & Payne,

2009b). Furthermore, it is deemed best practice for this duty of care to extend into the phases of post-patient death and bereavement (Palliative Care Australia, 2005; Relf, Machin, & Archer, 2008). In recent years, the importance of developing and identifying support interventions for caregivers involved in terminal care has been recognised by a number of health care agencies and research bodies (Candy, et al., 2009; Eagar et al., 2007; Palliative Care Australia, 2004). Despite the evidence of caregiver burden, there are minimal evidence based strategies or interventions to ensure effective delivery of support to caregivers and families of palliative care patients.
While the national standards for palliative care services endorse this principle in many countries (Relf, et al., 2008), it is not always feasible to provide care for all family members of a palliative care patient. In an effort to set realistic objectives in the provision of palliative care, it has been recommended that support should focus on the needs of primary caregiver(s) in the first instance and where resources allow, the entire family (P. Hudson & Payne, 2009b; Relf, et al., 2008). Primary caregivers) usually provide primary support for the patient at all levels of need. They may be the patient‟s spouse, child, another family member or a friend. Although the primary caregiver may be supported by other caregivers, they generally assume primary responsibility for the co-ordination and provision of care and support to the patient (Palliative Care Australia, 2005)
Ways to Cope with the Loss of a Loved OneRelationship with the dead person and manner of death can also influence the
grieving process. Even if the death was expected as in cases of terminal illnesses where families may have undergone ‘anticipatory grief’ and are supposedly prepared for the loss, facing the reality of death can still be traumatic. The suffering undergone before death also increases the pain and sorrow of the bereaved.
The loss of a spouse can be extremely traumatic. For some, it can be life-changing, especially if the spouse was the sole breadwinner, which can bring both emotional as well as financial stress on the bereaved spouse.
The loss of a child is by far the worst form of grief. It can send parents into a state of deep shock and denial. Grief over the loss of a child is also accompanied by guilt, a sense of injustice and anger, and also wishes of what could have been if the death was averted. Memories of the precious one could haunt ceaselessly, making it one of the toughest bereavements to cope with.

Unexpected deaths due to accidents or suicide, or even a sudden illness can also be very difficult to cope with. The bereaved experience extreme guilt, and may blame themselves for the situation especially in cases of death by suicide where they feel the death could have been prevented. Accepting the loss of a loved one in such cases may take longer.
Multiple deaths within a family can also exacerbate grief making it very tough for those left behind. An acute sense of shock envelops the aggrieved, who could go through stress, trauma, anxiety and depression. Professional help and counseling may be the best way to deal with such trauma.
Risk Factors for Complicated Grief and Other Negative Bereavement Outcomes
One study of 248 caregivers of terminally ill cancer patients investigated the presence of pre-death complicated grief and its correlates. Results revealed the following variables associated with higher levels of pre-death complicated grief:
• Age younger than 60 years.• Lack of perceived available social support.• History of depression and current depression.• Lower income.• Pessimistic thinking.• Severity of stressful life events.
Of these correlates, pessimistic thinking and severity of stressful life events were independent predictors of pre death complicated grief.
Other research has focused on predictors of outcomes such as symptoms of depression and overall negative health consequences. Three categories of variables have been investigated:
• Situational (e.g., circumstances of the death).• Personal (e.g., personality characteristics, gender).• Interpersonal context (e.g., social support, kinship).
Most research has focused on spousal/partner loss and is not uniquely focused on death via cancer.
Situational: Expected or Unexpected Death
Although theory suggests that a sudden, unexpected loss should lead to more difficult grief, empirical findings have been mixed. The impact of an unexpected loss

seems to be moderated by self-esteem and perceived control: Bereaved persons with low self-esteem and/or a sense that life is uncontrollable seem to suffer more depression and somatic complaints after an unexpected death than do bereaved persons with higher self-esteem and/or a sense of control.
Personal: Personality Characteristics
Attachment theory has suggested that the nature of one’s earliest attachments (typically with parents) predicts how one would react to loss. Bereaved persons with secure attachment styles would be least likely to experience complicated grief, while those with either insecure styles or anxious-ambivalent styles would be most likely to experience negative outcomes.
In a study of 59 caregivers of terminally ill spouses, the nature of their attachment styles and marital quality were evaluated. Results showed that caregivers with insecure attachment styles or in marriages that were "security-increasing" were more likely to experience symptoms of complicated grief. Persons with a tendency toward "ruminative coping," a pattern of excessively focusing on one’s symptoms of distress, have also been shown to experience extended depression after a loss.
Personal: Religious Beliefs
Theory has proposed that strong religious beliefs and participation in religious activities could provide a buffer to the distress of loss, via two different mechanisms:
• A belief system that helps one cope with death.• A network of social support that comes with religious participation.
However, empirical results about the benefits of religion in coping with death tend to be mixed, some showing positive benefit and others showing no benefit or even greater distress among the religious. Studies that show a positive benefit of religion tend to measure religious participation as regular church attendance and find that the benefit of participation tends to be associated with an increased level of social support. Thus it appears that religious participation via regular church attendance and the resulting increase in social support may be the mechanisms by which religion is associated with positive grief outcomes.
Personal: Gender
In general, men experience more negative consequences than women do after losing a spouse. Mortality rates of bereaved men and women are higher for both men and

women compared to no bereaved people; however, the relative increase in mortality is higher for men than for women. Men also tend to experience greater degrees of depression and greater degrees of overall negative health consequences than do women after a spouse’s death. Some researchers have suggested that the mechanism for this difference is the lower level of social support provided to bereaved men than that provided to bereaved women.
Personal: Age
In general, younger bereaved persons experience more difficulties after a loss than do older bereaved persons. These difficulties include more severe health consequences, grief symptoms, and psychological and physical symptoms. The reason for this age-related difference may be the fact that younger bereaved persons are more likely to have experienced unexpected and sudden loss. However, it is also thought that younger bereaved persons may experience more difficulties during the initial period after the loss but may recover more quickly because they have more access to various types of resources (e.g., social support) than do older bereaved persons.
Interpersonal Context: Social Support
Social support is a highly complex construct, consisting of a variety of components (perceived availability, social networks, supportive climate/environment, support seeking) and measured in a variety of ways. However, as mentioned above, lack of social support is a risk factor for negative bereavement outcomes: It is both a general risk factor for negative health outcomes and a bereavement-specific risk factor for negative outcomes after loss. For example, after the death of a close family member (e.g., spouse), many persons report a number of related losses (often unanticipated) such as the loss of income, lifestyle, and daily routine—all important aspects of social support.
REVIEW OF LITRETURE:
1. Rodie Akerman and june stataham (2011)
This rapid review has considered evidence for the impact of childhood bereavement on educational and psychological outcomes for children, and the effectiveness of services to support bereaved children. Most children do experience some negative impact on psychological wellbeing in the short term (up to a year) from bereavement of a parent or sibling, but for the majority of

children these difficulties do not persist or require specialist intervention. Evidence of impact on educational attainment is generally lacking. There is also little hard data on long-term outcomes from parental bereavement in childhood, although a new analysis of the 1970 birth cohort study suggests that there may be some impact, particularly for women, on outcomes at age 30 such as having any qualification, being employed, having symptoms of depression or being a smoker.
2. St. Joseph’s Hospice, Hackney/
St. Christopher’s Hospice, Sydenham, UK (2011)
Much of the writing on the subject of bereavement during the first three quarters of the twentieth century were written from the point of view of western psychiatrists. As such it presented a reasonably consistent view but one limited by a frame of reference which has been primarily concerned to identify risks to mental health and prevent psychiatric problems. More recently psychologists, sociologists, anthropologists, clergy and non-psychiatric health care staff have carried out their own studies and developed their own theories. Many of these will be found in the papers published in ‘Mortality’ since its inception in March 1996, they include some of the most influential voices in current European thanatology. Each of them has made their own unique contribution to our understanding of the wide topic of bereavement. The multiplicity of view points and the natural tendency for writers to see their own perspective as superior to that of others, may create confusion and I would like to take this opportunity to attempt a synthesis of views which I regard as complementing more often than undermining each other.
3. Dr Cheryl Remedios, Dr Kristina Thomas and Professor Peter Hudson(2011)

Caregivers of palliative care patients face complex and challenging tasks including physical, medical, financial, legal and emotional aspects of care giving. While many caregivers report that care giving provides positive and valuable experiences, a high proportion of caregivers report considerable burden on their own physical health, psychological well-being, financial welfare and social life. It is recommended that the assessment of caregivers‟ needs and well-being become routine in palliative care.
Greater recognition of the factors that increase or decrease caregivers‟ vulnerability for burden is advocated. Risk factors for psychological burden include sleeplessness, higher levels of caregiver esteem, financial difficulties, greater impact on schedules, greater impact on health and pessimistic thinking. Protective factors that decrease caregivers‟ vulnerability for burden include involvement in previous commitments, setting limits and boundaries, adequate personal and professional support, participation in valued activities and an optimistic outlook on life.
4. Lord Freud (2011)
Initial findings indicate that: for most people, regardless of household income or whether or not they are in work, the death of a working age spouse or civil partner has a significant financial impact, which is particularly acute in the few months following bereavement; longer term financial impacts were more varied, with an apparent correlation between being outside the labour market and having significant ongoing financial needs; and decision making can be very difficult in this period. Most people found bereavement benefits extremely valuable, but some felt they could be enhanced by greater interaction from government throughout the payment period, to provide sensitive employment support and reiterate practical information about the benefit at a time when it can be more easily absorbed. Respondents who were less positive about bereavement benefits had often received other state benefits at the time of bereavement and noted that bereavement benefits caused these other payments to be reduced.

5. Louise Casey CB (2011)
For most families the criminal justice process is unknown and their state of vulnerability makes it difficult and unreasonable for them to negotiate this themselves. Because there are a series of competing interests within that justice process, the rights of bereaved families can be overlooked. Those working with bereaved families who are not part of the criminal justice process – including the national homicide service caseworkers, volunteers and peer support groups – should know what families are entitled to expect and to challenge shortcomings. The system needs some challenge to ensure that it is taking account of the families’ reasonable and legitimate needs
6. Susan Allen Professor Stephen Brown (Chair) (2011)
SUDEP is when a person with epilepsy dies suddenly and no other cause of death is found. There are over 1000 epilepsy-related deaths each year in the UK, of which over 500 are attributed to SUDEP. “It is a privilege to be working with such a strong and necessary charity. For many years hundreds of people were dying of unexplained death related to epilepsy and it took effort and courage to bring this into national focus. As a result we now more fully understand the problem and the impact and I am sure that the scientific basis of this work will save many lives in the future as the wonderful support for families tries to reduce the pain of bereavement”.
7. Monica Flexhaug, BSc, MHS
Erdem Yazganoglu, MD, MA, MHSc (2009)

Most of the above tools were developed to be applied in clinical assessment, and in a clinical environment, and most have been used with general bereaved populations. These tools have not been tested for implementation in a community environment through lay facilitators. Furthermore, the capability of the community organizations to analyze this data and apply it in decision making and service improvements may be limited. Among the grief instruments, the Grief Experience Questionnaire is the one most suited to identify grief experiences of suicide survivors. Although this instrument shows the ability to separate the grief experiences of survivors from other forms of grief, the ability of the tool to show differences between test-retest have not been assessed. Therefore, it was not recommended to be used in clinical applications.
8. Ms Jodie Croxall & Dr Sarah Hillcoat-Nalletamby. IAGG (2009.)
Preliminary analysis suggests that social isolation and loneliness are particularly dominant concerns amongst older bereaved people. Social change (e.g. increasing divorce, women in work etc) affects the availability of informal support. older people interviewed felt that they have particular unmet needs for support following bereavement, especially with practical matters (such as paperwork, funeral arrangements); functional support (such as transport, shopping, cleaning); emotional support. (companionship; somebody to talk to) and empathetic support (shared bereavement experiences)
9. Janet Leckey (2008)
Cruse Bereavement Care in Northern Ireland is part of a national organisation which promotes the well-being of bereaved people and to enable anyone bereaved by death to understand their grief and cope with their loss. Cruse has 24 years experience of providing bereavement support in Northern Ireland and the wide range of services are provided free of charge. The services are available to adults

and children aged 4 – 18 years, delivered by trained volunteers to respond to all causes of bereavement. Currently there are over 500 volunteers involved in activities including management committee membership, supervision, administration, fundraising training and vital face to face support and counselling.
10.By Helen E. Benedict, PhD, RPT-S (2008)
There are two major categories of death experiences: uncomplicated and complicated bereavement. Complicated bereavement can be further divided into death complicated by stigma and traumatic death. Uncomplicated bereavement is defined as the normal grieving process when one experiences the loss of an important relationship. It is noteworthy that with uncomplicated bereavement, children who are adequately parented following the death do not appear to be at risk of later mental illness. In both types of complicated bereavement, especially traumatic grief including PTSD, there is heightened risk for later development of significant psychopathology
11.Aberdeen (2007)
The majority of materials in this section are observational studies or opinion pieces (evidence ratings are predominantly in the 3-4 level) that seek to establish distinctions between complicated grief and other diagnoses. Presently, it would appear that, there is no accepted diagnosis of complicated grief unless it is related to other mental health diagnoses. Therefore, those who are bereaved with signs and symptoms of complicated grief are often diagnosed with anxiety and depression or Post Traumatic Stress Disorder (PTSD), which may, or may not, be appropriate.
12.Sharon Begley (2007)

In recent years there has been considerable interest in the effectiveness of psychotherapies including grief counseling and therapy. With regard to the impact of mental health treatment for grief, two issues have come to the forefront: the efficacy of grief counseling and a claim that grief counseling can actually be harmful. The Association for Death Education and Counseling (ADEC) sees the question of efficacy as a significant research challenge, made more complex by variations in methodologies, analytic stances, and preferred approaches toward the vulnerable population of mourners. It is important to note that the question of harm is an ancillary issue within an investigation of overall efficacy.
13.Palliative Medicine 2007
Still, there is conflicting evidence as to whether religion helps in the process of coping with loss. Research has demonstrated many positive attributes of religion at the end of life and during stressful life events. The causes of death were also various, including death of illness (especially cancer), suicide, homicide, stillbirth, neonatal death, violent deaths and accidents. Range of time since death of the deceased was between 1 month and 41 years.
14.Heather Gaines Hardison, Robert A. Neimeyer,
and Kenneth L. Lichstein (2005)
Insomnia has been commonly associated with bereavement. Thus, on the one hand, bereavement researchers have reported that grief is linked to impairments in sleep (Prigerson, Frank, et al., 1995), and on the other hand, sleep researchers list bereavement among the common causes of insomnia (Lichstein & Reidel, 1994). Despite this recognition of the mutual relevance of sleep and bereavement studies, the relation between sleep disturbance and grief symptomatology has received

surprisingly little systematic attention. The goals of this study were to establish the frequency of insomnia and associated sleep behaviors among a large cohort of bereaved young adults and to investigate their relation to complicated grief symptomatology.
15.Hannelore wass Jane E. Myers (2005)
Death is inescapable fact of life that touches everyone at sometime. So all counselors regardless of their work setting will be faced with mindset to help someone adjust to death, whether their own or a death of a parent, spouse, child or friend. Help older persons cope with death may be made easier for those counselors who are familiar with the known psychosocial aspect of death among elderly.
16.Joseph M. Currier, Jason M. Holland, and Robert A. Neimeyer (2005).
The overall results do not support the assumption that the bereavement interventions with children have a significant influence on adjustment. On average, the treated child did not appear to be better than bereaved children who did not participate in grief therapy. The results of our review lead to the same general conclusion, namely that the interventions with bereaved children do not appear to produce the outcomes that are expected from professional psychotherapeutic interventions.
17.Mary McClain, RN, MS Joan Arnold, RN, PhD Evelyne Longchamp, RN, MA Jodi Shaefer, RN, PhD(2004)

Key to the development of effective skill as a bereavement counselor is the willingness
to seek personal insight and gain objectivity about one’s motivation to do this work. Every person has a history of loss, and has processed loss in unique ways influenced by the nature of his or her relationships, family dynamics and cultural context. The history and processing of loss provide a foundation of experience, and issues emanating from personal experiences of loss tend to be played out in the helping context. It is imperative, therefore, that the bereavement counselor seeks insight and gains objectivity about personal experiences of loss in order to achieve objectivity in the therapeutic relationship with bereaved parents and others.
18.Palliative Medicine (2003)
The death of a loved person is a normal part of life, one that at first sight may not be an obvious topic for scientific investigation. Is it not enough to rely on human insight and clinical experience to provide the right sort of support for bereaved people and to understand grief and grieving? In fact, there are a variety of arguments that can be given in support of an empirical, scientific approach, from both societal and theoretical points of view, but let us instead take an apparently simple example that turns out to be more complex than expected.
19.Boston, MA(2003)
If the family is resistant to the idea of autopsy, the physician or nurse may be able to alleviate anxiety associated with this procedure. First, it is helpful to explain to parents that an autopsy is a medical procedure similar to surgery or an "operation". A specialized physician or pathologist performs this operation in a respectful manner. Second, besides ruling out injury, an autopsy will eliminate or confirm any unsuspected illness or congenital anomaly as the cause of death.

Third, in almost all cases in which autopsies are not performed, the family may have lingering doubts as to the cause of death.
20.The Community Advisory Panel (CAP)(2002)
The bereavement process is very individual. As such the needs of relatives will differ on a case-by-case basis. It is noted that the needs will also be affected by how sudden or expected the death of the patient was.
In general, the CAP were very satisfied that the bereavement process is organised and ‘fit-for-purpose’. It should be noted that only the RVI and Freeman sites were considered. A number of observations and suggestions for improvements are made.
Both the bereavement offices and mortuary viewing facilities were felt to be accessible to users, though the approach to the viewing facility at the Freeman is far from ideal (in the basement, on a noisy service corridor which can be dark due to the movement sensitive lighting).
21.Margaret Stroebe, Henk Schut, Wolfgang Stroebe(2002)
People who have been bereaved are more likely to have physical health problems, particularly those who have been bereaved recently. Bereaved individuals also have higher rates of disability, medication use, and hospitalization than non-bereaved counterparts. Although widowed people in general consult with doctors more frequently, most likely because of symptoms of anxiety and tension,35 findings suggest that many of those with intense grief might fail to consult with doctors when they need to.

22.Jennifer Holliday (2002)
In many cases, there is no evidence of significant increases in psychological morbidity associated with sibling bereavement. However, both internalizing and externalizing problems may emerge in situations where: traumatic death has occurred the family has difficulty adjusting predisposing factors such as previous depression are present The secondary effects of sibling bereavement may have a more profound impact on the surviving child. Such as: loss of the sibling relationship change to the role the sibling plays within the family
23.Elizabeth Templeton (2000)
Teachers are in an ideal situation, without the personal burden of the child’s loss, to help grieving students feel safe, acknowledge that their loss is real, provide an environment for sharing feelings and structure learning experiences to deal with grief and loss circumstances (Charkow, 1998). With specialist training, school counselors are able to provide additional support for grieving students through individual and or group therapy, family intervention and development of identification and referral processes and school grief and loss programs
24.St. Joseph’s Hospice, Hackney/ St. Christopher’s Hospice, Sydenham (2000)
All in all it would appear that we now have a great deal of knowledge about the nature of bereavement and its consequences. If there were ever counsellors who confined themselves to aiding in the expression of emotions (as Walter maintains but Stroebe, McLaren and Footman disagree), this can no longer be the case. There seems to be general agreement that bereaved people need to talk there way through

grief. As Walter puts it, the helper can share in ‘the never-ending and reflexive conversation with self and others through which the late-modern person makes sense of their existence’. It is time to put aside minor academic differences and get on with the job of caring.
25.John Hinton (2000)
Prepare for the death of someone you are close to. It is important emotionally and practically to talk things over. If you are preparing for the death of your partner, discuss with them the jobs your partner used to do, sort out finances. Say all the things you would want to say. Carefully consider whether you want to see the body of the dead person. Some people may feel this is too distressing but can regret it later on if they have not done this. Follow your own feelings. There is no right or wrong thing to do, but do think it out. Funeral arrangements should be considered carefully. Try to have someone with you. Don’t feel pressured into a funeral that is too expensive for your budget. Try and think about what you really want.
RESEARCH METHODOLOGY
Introduction
Research is common terms refer to the research for knowledge. One can also define research as a scientific and systematic search for information on a specific topic. In fact research is an art of scientific investigation. Roadmann and Morry (1923) defined research as a systematic effort to gain knowledge. It is the pursuit of truth with a help on

study, observation, comparision and experiment through objective and systematic methods of finding solution to a problem. Research is, thus an original contribution to the existing stock of knowledge making for its advancement.
Research is defined as “a systematized effort to gain new knowledge”. The word research itself gives the meaning as re-searching, searching for more relevant facts from the existing facts. It refers to the systematic method consisting of enunciating problem, formulating hypothesis, collecting facts and reaching certain conclusion, either in the form of solution towards the concerned problem or in central generalization for the same theoretical formation. It can be defined as a careful critical inquiry or examination in seeking facts or principles and to design investigation in order to ascertain something. Research methodology prepares the investigator to adopt techniques and tools to neutralize the effect of hurdles. It is description, explanation and justification of various methods of continuing research.
Research methodology is an important part of a specific study. Every researcher should have a well-defined methodology, which states the relevance of the study.
Formulation of research problem
After reviewing a number of articles and literatures, the researcher was able to understand that many study were conducted to measure the level of bereavement among children’s, spouse etc,. There is very little research study in this area, so the researcher was interested in carrying out a study on the level of bereavement among care givers of hospice patient.
Need:
Caregivers are facing lots of problems like sorrow, grief, pain, suicidal tendency with bereavement. Especially care givers of hospice patients have more pain after the loss of their loved one, so there is a need to study about the bereavement among the care givers of hospice patients.
Scope:

People cope with the loss of a loved one in many different ways. For some, the experience may lead to personal growth, even though it is a difficult and trying time. There is no right or wrong way to cope with the passing of a loved one. The way a person grieves depends on the personality of that person and the relationship with the person who has died. How a person copes with grief is affected by many factors: the person's experience with the illness, the way the disease progressed, the person's cultural and religious background, his or her coping skills and mental history, existing support systems and the person's social and financial status. So there is more scope to study about the bereavement of a care givers of hospice patients.
Pretest
The pretest was conducted preliminary step to test the feasibility of the study. Find the extend of the cooperation of the respondents. Decide on the procedures and tools of data collection. As the pretest proved to be successful the researcher decided to go ahead with data collection.
Aim and objective(s):
Aim:
• To measure the level of bereavement among caregivers of hospice patients
Objective:
• To know how much the care givers have affected after the loss of their loved ones• To know how much the care givers have distressed after the loss of their loved
ones
• To know how much they missing them and how they coping their sorrow level.
Hypothesis:

• There is no significant difference with age of the care giver with regard to the level of bereavement
• There is no significant difference with sex of the care giver with regard to the level of bereavement
• There is no significant difference with Marital status of the care giver with regard to the level of bereavement
• There is no significant difference with Residence of the care giver with regard to the level of bereavement
• There is no significant difference with domicile of the care giver with regard to the level of bereavement
• There is no significant difference with Occupation of the care giver with regard to the level of bereavement
• There is no significant difference with Type of family of the care giver with regard to the level of bereavement
• There is no significant difference with Religion of the care giver with regard to the level of bereavement
Operational definition:
Bereavement
Bereavement is the level of psychological pain caregiver is having after the death of the hospice patient.
Caregiver
Care giver is the person who has taken care of hospice patients during hospitalization
Design of the study:
The research design is a plan of action indicating the specific steps that are necessary to provide answers to those questions, test the hypotheses, and thereby achieve

the research purpose that helps choose among the decision alternatives to solve the management problem or capitalize on the market opportunity
The researcher has used Diagnostic research design to find how much care givers are affected after the death of the hospice patient
About the Universe:
The researcher has selected CMS Pushpalaya charitable trust, Nellikkampoil for the research study. The universe consists of 200 caregivers of hospices
Inclusion criteria:
• Only Hospice patients alone included in this study.
Sampling procedure:
Researcher has used convenient sampling
Method of data collection:
The researcher has used Questionnaire method
Tools of data collection:
The researcher has adopted “ Bereavement Scale (Burnett, Paul C (1997)”. Bereavement scale is having 35 questions with 4 point and 5 point scale. First 32 questions will be having 4 point scale and rest of the 3 scales will be having 5 point scale.
Pretest
Standardized scale and socio demographic profile was pretested with 5 respondents
Statistical analysis
The researcher has used ‘t’ test and ANOVA to find the difference between age,
sex, marital status, Religion, Residence, Occupation, Type of family and domicile with
the level of bereavement among caregivers of hospice patients.

Difficulties faced by the Researcher
• The researcher faced some difficulty obtaining permission from the Charitable trust.
• The researcher has to visit the Charitable trust frequently to get information since the respondents were busy with their own works.
• The researcher faced the difficulty in communicating to the care givers as they are very much sad in the loss of their loved ones.
• Some of the care givers stopped in half way while filling up the questionnaire as they go back to the memories about their loved ones.
Limitations of the study
• The study is conducted only in CMS Pushpalaya Charitable trust, Nellikkampoil, so it cannot be generalized.
Chapterization

Chapter I
Part A
This chapter contains the introduction of Bereavement
Part B
This chapter contains the views of various different scholars and authors on Bereavement and related aspects, as a whole it is summed up as review of literature.
Chapter II
This chapter contains the research methodology of the projectChapter III
This chapter contains the analysis and interpretation of the collected data.
Chapter IV
This contains the findings, suggestion, conclusion, bibliography and appendix of the project.
Data analysis and interpretation

Distribution of the respondents by their age
S.No Age Frequency Percentage
1 25 - 35 5 8.3
2 35 - 45 18 30.0
3 45 - 55 11 18.3
4 Above 55 25 43.0
Total 60 100
Table 1 indicates the distribution of respondents by their age. It can be observed that among the total respondents 8.3 belongs to age of 25 – 35 , 30.0% belongs to age of 35 – 45, 18.3 %belongs to age of 45 – 55, 43.0% belongs to above 55.

Distribution of the respondents by their age
Distribution of the respondents by their sex
S.No Sex Frequency Percentage

1 Male 10 16.7
2 Female 50 83.3
Total 60 100.0
The above table reveals those majorities 48% of the respondents belong to the age group of 26 to 33 years,33% of the respondents belongs to the age group of 18 to 25 years,10% of the respondents belong to 34 to 41 years, 6% of the respondents belong to 42 to 49 years, 3% of the respondents are above 50 years.
Distribution of the respondents by their sex

Distribution of the respondents by their Marital Status

S.No Marital Status Frequency Percentage
1 Married 5.7 95.0
2 Unmarried 3 5.0
Total 60 100.0
Table 3 indicates the distribution of respondents by their marital status. 95.0 % of them are married, 5.0 % of them are unmarried.
Distribution of the respondents by their Marital Status

Distribution of the respondents by their Marital Status

S. No Religion Frequency Percentage
1 Hindu 30 50.0
2 Christian 23 38.3
3 Muslim 7 11.7
Total 60 100.0
Table 4 shows the distribution of respondents by their religion. 50.0 % of them are Hindus, 38.3 % are Christians and 11.7 % of them are Muslims.
Distribution of the respondents by their Marital Status

Distribution of the respondents by their Occupation

S.No Occupation Frequency Percentage
1 Farming 23 38.3
2 Others 37 61.7
Total 60 100.0
Table 5 indicates the distribution of respondents by their type occupation. 38.3 % of them are farmers and rests of them are not farmers.
Distribution of the respondents by their Occupation

Distribution of the respondents by their Domicile

S.No Domicile Frequency Percentage
1 Rural 53 88.3
2 Urban 7 11.7
Total 60 100
Table 6 depicts the distribution of respondents by their domicile. It can be observed that among the total respondents 88.3% are belongs to rural domicile and 11.7% are belongs to urban
Distribution of the respondents by their Domicile

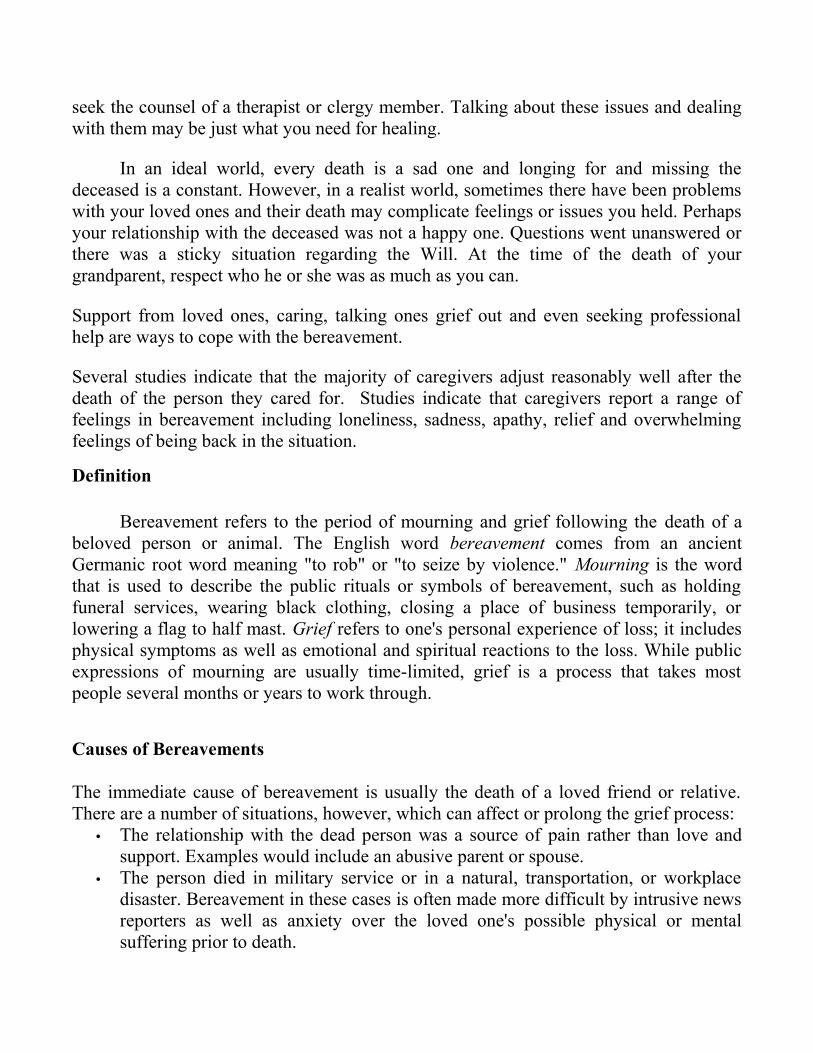
Distribution of the respondents by their Residence

Residence Frequency Percentage
Own 37 61.7
Rental 23 38.3
Total 60 100.0
Table 7 indicates that whether the respondent having an owned or rental residence.
61.7% of them are having own houses and the rest are having rent houses.
Distribution of the respondents by their Residence

Berevement
LevelFrequency
Percent
Valid Percent
Cumulative Percent
Valid 1 6 10.0 10.0 10.0
2 27 45.0 45.0 55.0
3 27 45.0 45.0 100.0
Total 60 100.0 100.0
The above table reveals that 45% of the respondents are having moderate level of
bereavement, 45% of the respondents having High level of bereavement and 10% of the
respondents having low level of bereavement.
.

Bereavement

Distribution of the respondents by their Type of family
S.No Type of Family Frequency Percentage
1 Joint Family 48 80
2 Nuclear Family 12 20
Total 60 100.0
Table 8 shows the distribution among respondents based on their type of family. In that 80% of them are belongs to joint family and 20% of them are belongs to nuclear family.

Distribution of the respondents by their Type of family

One-way Analysis of variance among the age of the respondents with regard to their level of bereavement
MeanSum of square
DFMean of Square
FStatistical inference
Between Groups
G1=2.60G2=2.28G3=2.36G4=2.35G5=2.35
.409 3 .136 .302 P=.824
Within Groups
25.241 56 .451
P>. 05
No significance
G1= 25 to 35; G2=35 to 45; G3=45 to 55; G4= above 55
Hypothesis: 1
There is no significant difference between Age of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Hence the hypothesis 1 is accepted.
There is no significant difference between the mean score (2.60) indicates that the above 25 to 35 Age group respondents have more Bereavement.

Student’s t-test between the Sex of the respondents with regard
to their level of Bereavement
Sex N Mean Std. Deviation t-valueMale
Female
1050
2.602.30
0.5160.678
T= .133P > .05No significance
Hypothesis: 2
There is no significant difference between Age of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Hence the hypothesis 2 is accepted.
There is no significant difference between the mean score (2.60) indicates that the above Male respondents have more Bereavement.

Student’s t-test between the Marital Status of the respondents with regard to their level of Bereavement
Marital Status N Mean Std. Deviation t-valueMarried
Un married
57
3
2.33
2.67
0.664
0.577
T= .424P > .05No significance
Hypothesis: 3
There is no significant difference between Marital Status of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Marital Status of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.424), which is significant at 0.05 levels.
Hence the hypothesis 3 is accepted.
There is no significant difference between the mean score (2.67) indicates that the above Un married respondents have more Bereavement.

One-way Analysis of variance among the Religion of the respondents with regard to their level of bereavement.
MeanSum of square
DFMean of Square
FStatistical inference
Between Groups
G1=2..37G2=2.30G3=2.43 0.099 3 .050 .111 P=.895
Within Groups
25.551 57 .448
P>. 05
No significance
G1= Hindu; G2=Christian; G3=Muslim
Hypothesis: 4
There is no significant difference between Religion of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Religion of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.895), which is significant at 0.05 levels.
Hence the hypothesis 4 is accepted.
There is no significant difference between the mean score (2.43) indicates that the above Muslim respondents have more Bereavement.

Student’s t-test between the Occupation of the respondents with regard to their level of Bereavement
Occupation N Mean Std. Deviation t-valueFarming
Others
23
37
2.35
2.35
0.647
0.676
T= 0.984P > .05No significance
Hypothesis: 5
There is no significant difference between Religion of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Religion of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.984), which is significant at 0.05 levels.
Hence the hypothesis 5 is accepted.
There is no significant difference between the mean score (2.35) indicates that the above Farming and other occupation respondents have more Bereavement.

Student’s t-test between the Domcile of the respondents with regard to their level of Bereavement
Domicile N Mean Std. Deviation t-valueRural
Urban
53
7
2.28
2.86
0.662
0.378
T= 0.006P > .05No significance
Hypothesis: 6
There is no significant difference between Religion of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Religion of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.006), which is significant at 0.05 levels.
Hence the hypothesis 6 is accepted.
There is no significant difference between the mean score (2.86) indicates that the above urban respondents and other occupation have more Bereavement.

Student’s t-test between the Type of family of the respondents with regard to their level of Bereavement
Type of family N Mean Std. Deviation t-valueJoint family
Nuclear family
48
12
2.40
2.17
0.644
0.718
T= 0.328P > .05No significance
Hypothesis: 7
There is no significant difference between Religion of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Religion of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.328), which is significant at 0.05 levels.
Hence the hypothesis 7 is accepted.
There is no significant difference between the mean score (2.40) indicates that the above Joint family respondents have more Bereavement.

Student’s t-test between the Residence of the respondents with regard to their level of Bereavement
Residence N Mean Std. Deviation t-valueOwn
Rental
37
23
2.35
2.35
0.647
0.676
T= 0.984P > .05No significance
Hypothesis: 8
There is no significant difference between Residence of the respondents with regard to their Level of Bereavement
It is inferred from the above table that there is no significant difference between the Residence of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.984), which is significant at 0.05 levels.
Hence the hypothesis 8 is accepted.
There is no significant difference between the mean score (2.35) indicates that the above Own and Rental Residence respondents have more Bereavement.

Findings
Age
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Hence the hypothesis 1 is accepted.
There is no significant difference between the mean score (2.60) indicates that the above 25 to 35 Age group respondents have more Bereavement.
Sex
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Marital status
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Occupation
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Residence
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Religion

It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levelsDomicile
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels
Type of Family
It is inferred from the above table that there is no significant difference between the Age of the respondents with regard to their score in Bereavement. The calculated ‘F’ value is (0.824), which is significant at 0.05 levels.
Conclusion :

In the current world that is materialistic in all sense, bereavement has many levels of meanings. A scenario where people tend to be interdependent emotionally, physically & socially, bereavement has a very significant role in the day to day life.
This study itself is a proof that being intimate, any human being can develop emotional dependency towards each other. Being a social animal, man always has a tendency for mutual sharing and bereavement again is an outcome of this social characteristics.
Suggestions :
1. Each and every family members should give support to the hospices 2. Parents should teach children about how to behave to the hospices if they are in
family.3. Government must establish certain policies regarding their upliftment.4. All the hospitals taken care of hospices especially, nurses and other care givers try
to give them to mental moral support.5. Society should accept the hospices. If the hospices need any help the society
should try provide it.6. Moral support to the care givers in whatever ways possible.7. Special training programs to overcome the bereavement.8. Remember, with support, patience and effort, you will survive grief. Some day the
pain will lessen, leaving you with cherished memories of your loved one.

SCALES :BEREAVEMENT PHENOMENOLOGY SCALE Burnett, Paul C (1997)
This is a scale which measures a variety of attitudes feelings and behaviors among care givers of hospice patients. So please try very hard to completely honest in your answers. Results are confidential.Read each questions and place an (X) under the column which applies best for you.Please read each question carefully.
Thank you.
PERSONAL PROFILE
Name ……………………………… Date ……………….
Age ………………………………
Sex ………………………………(Male / Female)
Marital Status ………………………………(Single / Married)
Religion ………………………………(Christian / Hindu / Muslim / Others)
Occupation ………………………………(Farmers / Business / Others)
Domicile ………………………………(Urban / Rural)
Type of Family………………………………(Nuclear / Joint)
These questions ask about your experience in relation to the recent loss of your loved ones, whose name in these questions will be signified by the symbol ‘X’.
1. Do you experience image of the events surroundings X’s death ?
□ Continuously □ Quite a bit of time □ A little bit of time □ Never

2. Do thoughts of X come in to your mind whether you wish it or not ?
□ Continuously □ Quite a bit of time □ A little bit of time □ Never
3. Do thoughts of X make you feel distressed ?
□ Always □ Quite a bit of time □ A little bit of time □ Never
4. Do you think about X ?
□ Continuously □ Quite a bit of time □ A little bit of time □ Never
5. Do images of X make you feel distressed ?
□ Always □ Quite a bit of time □ A little bit of time □ Never
6. Do you find yourself preoccupied with images or memories of X ?
□ Continuously □ Quite a bit of time □ A little bit of time □ Never
7. Do you find yourself thinking of reunion with X ?
□ Always □ Quite a bit of time □ A little bit of time □ Never
8. Do you feel as though X is present ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
9. Do you at times feel as though you have seen X ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
10.Do you feel at times as though X has touched you ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
11.Do you at time as though you have heard X ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
12.When you dream about X does it feel as though X is still alive ?
□ Always □ Quite a bit of time □ A little bit of time □ Never
13.Do you currently recall dreaming about X ?

□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
14.Do you feel as though dreaming about X is helping you to cope with the loss ?
□ Always □ Quite a bit of time □ A little bit of time □ Never
15.Do you find yourself missing X ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
16.Are you reminded by familiar objects (photos, possessions, rooms etc.,) of X ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
17.Do you find yourself pining for / yearning for X ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
18.Do you find yourself looking for X in familiar places ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
19.Do you feel distressed / pain if for any reason you are confronted with the reality that X is not coming back ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
20.Do reminders of X such as photos, situations , music, places..you to feel longing for X ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
21.Do reminders of X such as photos, situations , music, places..you to feel loneliness ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
22.Do reminders of such as photos, situations, music, places etc., cause you to cry about X ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never

23.Do reminders of such as photos, situations, music, places etc., cause you to feel sadness ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
24.Do reminders of such as photos, situations, music, places etc., cause you to feel loss of enjoyment ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
25.Do reminders of such as photos, situations, music, places etc., cause you to feel dread ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
26.Do reminders of such as photos, situations, music, places etc., cause you to feel unreality ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
27.Do reminders of such as photos, situations, music, places etc., cause you to feel anxiety ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
28.Do reminders of such as photos, situations, music, places etc., cause you to feel numbness ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
29.Do reminders of such as photos, situations, music, places etc., cause you to feel guilt ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
30.Do reminders of such as photos, situations, music, places etc., cause you to feel anger ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never

31.Since X’s death how able are you to organize your life ?
□ Never □ A little bit of time □ Quite a bit of time □ A lot of time
32.Do you find you are able to organize life to your satisfaction ?
□ A lot of time □ Quite a bit of time □ A little bit of time □ Never
33.At the present time, do you feel able to assist others following X’s death ?
□ A lot less able to □ A bit less able to □ No change □A bit more able to □ A lot better able to
34.At the present time how do you feel having gone through the experience of X’s death ?
□A lot weaker □A bit weaker □No change □A bit stronger □A lot stronger
35.At the present time do you feel able to understand yourself following X’s death ?
□ A lot less able to □ A bit less able to □ No change □A bit more able to □ A lot better able to
_________________________________________

BIBLIOGRAPHY Bereavement : studies of grief in adult life
Colin Murray Parkes, Holly G. Prigerson - 2010 - 350 pages - PreviewLong recognised as the most authoritative work of its kind, this new edition is revised to take into account recent findings in the US and UK.
Bereavement : reactions, consequences, and care
Marian Osterweis, Fredric Solomon, Morris Green - 1984 - 312 pages - PreviewThey looked at rates of death and disease among bereaved persons; then they compared these rates with those for persons who had not lost a family member through death. What they learned generally lent scientific credence to what poets, ...
Bereavement
Dee Pilgrim - 2006 - 73 pages - PreviewThe guides are presented in a clear andaccessible manner and will help the reader to understandthe issue that they might be encountering and willprovide tips on how they can deal with it.
Bereavement : Words of Comfort in Times of Sorrow
James Serafina - 2008 - 58 pages - PreviewBereavement. Words of Comfort in Times of Sorrow is a book that offers support for the dying and those around them.
Dying, Death, and Bereavement
Lewis R. Aiken - 2001 - 398 pages - PreviewThis book is a brief but comprehensive survey of research, writings, and professionalpractices concerned with death and dying.
Death and bereavement across cultures
Colin Murray Parkes, Pittu Laungani, Bill Young - 1997 - 261 pages - PreviewThis book explores the richness of mourning traditions around the world with the aim of increasing the sensitivity and understanding which we all bring to the issue of death.
Bereavement : client adaptation and hospice services
Bereavement Counseling: Pastoral Care for Complicated Grieving
On bereavement : the culture of grief
Tony Walter - 1999 - 232 pages - Snippet viewThis ground-breaking book looks at the social position of the bereaved.
Counselling for Grief and Bereavement
Geraldine M. Humphrey, David G. Zimpfer - 2007 - 178 pages - PreviewIn Counselling for Grief and Bereavement, Second Edition Geraldine Humphrey and David Zimpfer take readers step-by-step through the skills needed to facilitate the process of grief, initiate healing, and promote a sense of growth
Bereavement : Counseling the Grieving Throughout the Life Cycle
David A. Crenshaw, William Van Ornum - 2002 - 181 pages - No preview
The Anatomy of Bereavement : A Handbook for the Caring Professions
Beverley Raphael - 1985 - 456 pages - PreviewBereavement is a painful and inevitable experience. This book shares the experience of many bereavements, how they are dealt with, understood, and eventually adapted to in the ongoing framework of human life.
Dying, Death, and Bereavement : A Challenge for Living
Inge B. Corless, Barbara B. Germino, Mary A. Pittman, DrPH - 2006 - 382 pages In this updated edition, the authors examine the issues of death and dying as a continuum, from death education and care of the dying to grief and bereavement.
Adolescent encounters with death, bereavement , and coping
David E. Balk, Charles A. Corr - 2009 - 390 pages - Preview" This new book, "Adolescent Encounters With Death, Bereavement, and Coping, " analyzes the challenges faced by adolescents coping with death, dying, and bereavement, and examines the new, unique circumstances and advances that have ...
Childhood bereavement : developing the curriculum and pastoral support
Nina Job, Gill Frances - 2004 - 70 pages - PreviewThis booklet aims to help teachers and those working in schools to support bereaved children and young people, and to communicate with all children and young people about death and dying.
Handbook of Bereavement : Theory, Research, and Intervention
Margaret S. Stroebe, Wolfgang Stroebe, Robert O. Hansson - 1993 - 546 pages - The Handbook of Bereavement constitutes a comprehensive review of scientific knowledge on the consequences of losing a loved person through death.
Children's encounters with death, bereavement , and coping
Charles A. Corr, David E. Balk - 2010 - 488 pages - Preview"[F]or the resource that offers one of the best bibliographies and guides to resources, for the book that contains theory, definitions, treatment modalities, helps, warnings, integration of people and programs, culural diversity...when it ...
Bereavement : reactions, consequences, and care : site visit case ...
Institute of Medicine (U.S.). Committee on the Health Consequences of the Stress of Bereavement, National Academy of Sciences (U.S.) - 1984 - 55 pages

Bereavement narratives: continuing bonds in the twenty-first century
Christine Valentine - 2008 - 193 pages - PreviewHowever, this empirically-grounded study argues that this is not always the best or only way to help the bereaved. in a radical departure, it emphasises normality and social and cultural diversity in grieving.
Loss and bereavement : managing change
Ros Weston, Terry Martin, Yvonne Anderson - 1998 - 268 pages - PreviewThis book encourages the use of range of skills while bringing a critical yet reflective dimension to this caring work. The text considers the work, school, family and social environments.
http://www.nhpco.org/files/public/InsightsIssue2_2003Social_Worker_pp8-9.pdf
http://www.nhpco.org/i4a/pages/index.cfm?pageid=3281
http://www.swlda.org/Summit.htm
http://www.swlda.org/Summit.htm
http://www.who.int/cancer/palliative/definition/en/
http://www.nhpco.org/files/public/InsightsIssue2_2003Social_Worker_pp8-9.pdf
http://www.nhpco.org/i4a/pages/index.cfm?pageid=3281
http://www.swlda.org/Summit.htm
http://www.swlda.org/Summit.htm
http://www.who.int/cancer/palliative/definition/en/

Social workers respect and integrate knowledge about how individuals and families are
influenced by their ethnicity, culture, values, religion- and health-related beliefs, and
economic situations. Social workers should understand systems of oppression and how
these systems affect client access to, and utilization of, palliative and end of life care.
Many cultures maintain their own values and traditions in the areas of palliative and end
of life care.
Culture influences individuals' and families' experience as well as the experience of the
practitioner and institution. Social workers should consider culture in practice settings
involving palliative and end of life care. Each cultural group has its own views about
palliative and end of life practices and these need to be understood as they affect
individuals' response to dying, death, illness, loss, and pain.
Social workers who understand how culture affects the illness and end of life experience
of an individual and family will be better able to individualize care and intervene in the
psychosocial impact of illness, pain, dying, and death. Therefore, social workers should
be familiar with the practices and beliefs of the cultural groups with whom they practice
to deliver culturally sensitive services.